 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
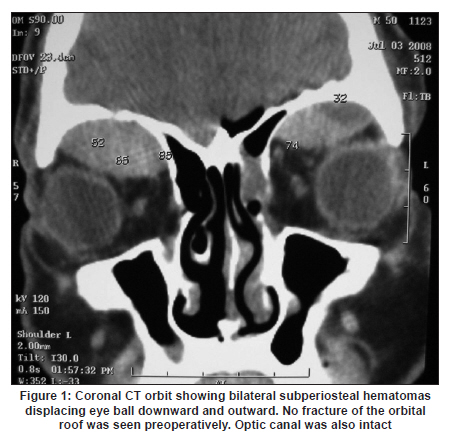
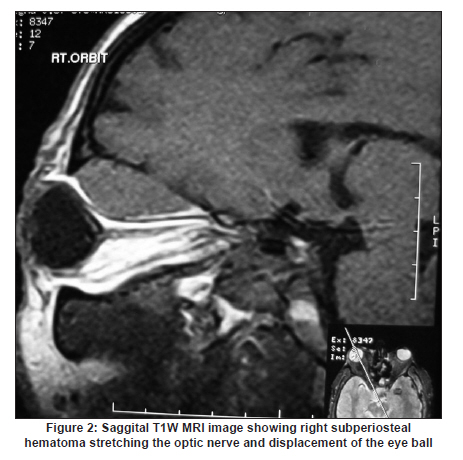
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 495-497 Letter To Editor Traumatic bilateral orbital subperiosteal hematoma with vision loss Rashim Kataria, Vimal Kumar, VS Mehta Division of Neurosurgery, Department of Neurosciences, Paras Hospital, Gurgaon - 122 002, Haryana, India Date of Acceptance: 01-Feb-2010 Code Number: ni10130 PMID: 20644294 Sir, Traumatic subperiosteal orbital hematomas are uncommon and bilateral occurrence is extremely rare and only one such case has been documented. Subperiosteal orbital hematomas are infrequently associated with visual loss, and when this occurs, it is often irreversible. We report one such uncommon case. A 50-year-old male, met with a road traffic accident following which he had a brief loss of consciousness. On regaining consciousness, he noted loss of vision in right eye. He was admitted to a regional hospital where he was given anticonvulsants, antiedema drugs and 36 h later was brought to our facility. His Glasgow coma score on admission was 15/15. Examination revealed a bruise and swelling in the right periorbital region with mild proptosis and restriction of right eye ball movements in all directions, maximum in superior gaze. There was no light perception in the right eye and he could count fingers at 4 feet with left eye. Pupil was 4.0 mm, not reacting to light on right side and was 3 mm reacting to light on left side. Visual field by confrontation method revealed no field defects in left eye. There was no pulsation or bruit. Coagulation profile and blood sugar values were within normal limits. Computerized tomography (CT) head scan revealed small interhemispheric subarachnoid hemorrhage (SAH) and droplet pneumocephalus in basal cisterns with fractures of left zygomatic arch and left squamous temporal bone. CT scan [Figure - 1] and magnetic resonance imaging (MRI) of the orbits showed bilateral subperiosteal hematoma (right > left) with indentation of the globe and stretching of optic nerve on the right side [Figure - 2]. He was given intravenous methylprednisolone immediately after admisson. Hematoma was evacuated by bilateral frontal craniotomy with de-roofing of the orbit. There was no evidence of frontal extradural hematoma or fracture of the orbit. No obvious bleeding point could be seen. The orbital periosteum appeared to be intact. Unfortunately he did not have any improvement in visual acuity in right eye at five months follow-up visit. There was no recordable visual evoked potential on right side. Subperiosteal hematoma of the orbit is an infrequent but well-described entity and reported as 'blood cyst' of the orbit in the earlier literature. [1] Bilateral lesions are even rarer. According to the location, orbital hematomas are classified as intraorbital or subperiosteal, the former being much more common. [2] Subperiosteal hematomas are seen in cases of direct orbital/facial trauma or after surgery in this region. Spontaneous hematomas are seen in patients with bleeding diathesis [3] or secondary to orbital venous congestion. Rarely they are secondary to frontal sinusitis. [4] They are also known to occur without bony injury. [5] Few cases have been reported as an extension of subgaleal hematomas in periorbital region. [6],[7],[8],[9] They are common in adolescents with male preponderance, ratio 4.5:1. [6] The mechanism of subperiosteal orbital hematoma is continuous bleeding from subgaleal vessels, which tends to dissect the periosteum from bone. Clinically, subperiosteal hematoma presents with painful, nonpulsatile proptosis and is due to eccentrically displaced globe. The globe displacement is usually downward and associated with upward gaze restriction as was seen in this patient also. Subperiosteal hematoma leading to visual loss is rare and, if present, it is usually irreversible and the visual loss is secondary to optic nerve/central retinal artery compression or retinal injury. [10],[11] Ecchymosis, which is the hallmark of intraorbital and retrorbital hematomas, is absent in subperiosteal hematoma. Subperiosteal hematomas are well visualized on CT as sharply defined hyperdense, extraconal nonenhancing mass with a broad base toward bone and displacing the periorbita centrally. [12] Other conditions which can produce painful proptosis after head injury include carotid cavernous fistula, retrorbital hematoma, post-traumatic thrombosis of cavernous sinus, orbital wall fracture, ocular AV-fistula and eye ball or extraocular muscle injury. [6],[7],[8],[9],[10],[11],[12],[13] When there is no visual loss, conservative treatment ranging from observation alone to topical use of temolol maleate, with or without oral acetazolamide, has been recommended. [1] In case of impending visual loss, urgent decompression of orbits and hematoma evacuation should be done. Needle aspiration may be successful in old liquefied hematoma, otherwise, orbital exploration and evacuation of the hematoma is required. Primary optic nerve injury can coexist with orbital hematomas and cannot be ruled out. It is quite possible that this patient might have had primary optic nerve injury, however, it is very difficult to prove or disprove it. Neurosurgeons should be aware of this uncommon entity, as good outcome may be expected if hematoma evacuation is done at an earliest. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10130f2.jpg] [ni10130f1.jpg] |
| |||||||||

{kind=link}
{kind=link}