 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
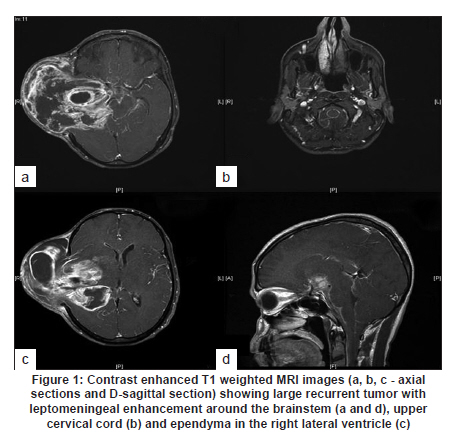
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 501-502 Neuroimage Florid leptomeningeal dissemination in a case of glioblastoma multiforme Prakash M Shetty, Aliasgar V Moiyadi Neurosurgical Services, Department of Surgical Oncology, Tata Memorial Hospital, Mumbai, India Date of Acceptance: 30-Nov-2009 Code Number: ni10133 PMID: 20644297 A 40-year-old male presented with a large right temporal swelling. He had undergone a right temporo-parietal craniectomy and biopsy for a temporo-parietal glioblastoma multiforme at an other facility and was advised radiotherapy, but had defaulted. Six months later he presented to us with a progressive lesion growing out of the cranial cavity. He had no neurological deficits despite the large recurrence. The magnetic resonance imaging (MRI) scan of the brain revealed a large tumor mass arising in the right temporo-parietal region with extension extra-cranially through the craniectomy defect. The lesion showed necrotic areas with inhomogeneous contrast enhancement. There was widespread meningeal enhancement seen along the brainstem, cerebellum, cervical cord, cerebral convexity and basal cisterns [Figure - 1]a-d. Ependymal enhancement was also seen in the right lateral ventricle [Figure - 1]c. The tumor was hyperperfused and had a spectral pattern consistent with glioblastoma multiforme. Debulking surgery was undertaken to facilitate the use of radiotherapy. However, extreme vascularity of the tumor and massive blood loss limited a radical resection. Histology revealed a classical glioblastoma. Patient developed hemi-paresis postoperatively and was referred for radiotherapy subsequently. Glioblastoma is the commonest primary malignant brain tumor in adults and most often spreads by local infiltration. Leptomeningeal spread through cerebrospinal fluid pathways as seen in primitive neuro-ectodermal tumors, ependymal tumors and germ cell tumors is rare in glioblastomas. The incidence of microscopic leptomeningeal spread in gliomas is reported as high as 30% at autopsy. However, most patients are asymptomatic. [1] and clinically significant leptomeningeal disease has been reported in only 1.55-4% of cases. [2] Few cases of leptomeningeal disease at initial presentation have been described, the majority being detected during treatment or at recurrence. Young age (usually less than 40 years), [3] incompletely excised or biopsied tumors (as in our case), and violation of the ependymal lining during surgery [4] are some of the risk factors associated with leptomeningeal spread. Leptomeningeal spread is associated with poor prognosis, with an average survival of 2.5 months after the diagnosis. [3] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10133f1.jpg] |
| |||||||||

{kind=link}