 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
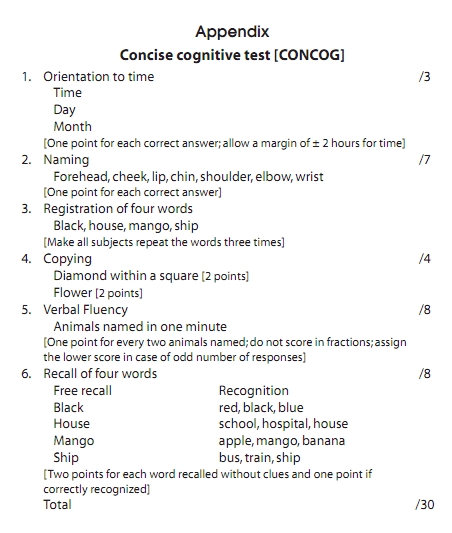
Neurology India, Vol. 58, No. 5, September-October, 2010, pp. 702-707 Original Article The concise cognitive test for dementia screening: Reliability and effects of demographic variables as compared to the mini mental state examination Srikanth Srinivasan Consultant Neurologist, Lanka Hospitals, Colombo, Sri Lanka Correspondence Address: Date of Acceptance: 11-Jul-2010 Code Number: ni10193 PMID: 21045491 DOI: 10.4103/0028-3886.72167 Abstract Background: The Mini Mental State Examination (MMSE) is widely used for dementia screening but has several shortcomings such as prominent ceiling effects, inadequate sensitivity to mild cognitive impairment, and uneven sampling of the major cognitive domains. Aims: In this study, we pilot a new dementia screening test - the Concise Cognitive Test (CONCOG) - designed to overcome the above short comings and describe the reliability measures and age, education, and gender effects. The CONCOG has a total score of 30, and has subtests for orientation, naming, registration, free recall and recognition of four words, semantic verbal fluency and copying. Patients and Methods: Participants were screened to exclude those with any neurological or psychiatric disease, simultaneously administered the CONCOG, and a Hybrid Mini Mental State Examination (HMMSE) adapted from Folstein's MMSE and Ganguli's Hindi Mental State Examination. Results: The study sample had 204 subjects over the age of 60 years with a mean of 73 years and education level of 8 (4.5) years. Internal consistency for the CONCOG (Cronbach's alpha) was 0.74, inter-rater reliability (Kendall's tau-b) was 0.9, and the one-month test-retest reliability (Kendall's tau-b) was 0.7. Age and education level, but not gender, significantly influenced performance on both scales. Although the influence of age on the two scales was to a similar degree, the HMMSE was more affected by education than the CONCOG. Of 204 subjects, only 12 (5.7%) subjects obtained the maximum score on the CONCOG compared with 30 (14.1%) subjects on the HMMSE. The CONCOG took less than 10 minutes to complete in this sample. Age and education stratified norms are presented for the CONCOG. Conclusions: The CONCOG is a reliable cognitive screening measure. It has negligible ceiling effects, is less influenced by education compared with the HMMSE, and offers subscale scores for the major cognitive domains. Keywords: Age, dementia, education, Mini Mental State Examination, screening Introduction Screening for dementia/cognitive impairment in the clinic requires an instrument that is brief, yet reliable. Despite universal use for this purpose, the Mini Mental State Examination (MMSE) [1] has many shortcomings such as insensitivity to mild and subcortical pattern of impairment, prominent ceiling effects, and uneven sampling of major cognitive domains. These concerns remain despite many translations and adaptations for populations with low literacy levels. [2],[3],[4] However, it has not been possible to stop using the MMSE because of its simplicity, brevity, and the absence of the need for specialized testing material. The need for an alternative to the MMSE has lead to the development of cognitive screening measures such as the Demtect, [5],[6] seven minute screen [7],[8],[9],[10] 7 MS, and the Montreal Cognitive Assessment. [11],[12],[13] Though these measures have demonstrated better sensitivity and specificity for diagnosing early dementia/mild cognitive impairment compared with the MMSE they take longer to administer, are more affected by education while some of them require complex test materials and are not easy to score. We collated well accepted cognitive screening items into the Concise Cognitive Test (CONCOG) to overcome the above shortcomings. Our main concerns were to keep the scale brief, simple, covering all major cognitive domains, and have minimal ceiling and educational effects. In this article, we describe the development, initial validation, and norming of the CONCOG in healthy elderly individuals. Patients and Methods Subjects After obtaining informed consent, all volunteering community-dwelling cognitively healthy elders were administered an initial screening interview and a clinical examination to exclude medical, neurological, or psychiatric illnesses that might affect cognition. All eligible subjects were then administered the CONCOG and the Hybrid Mini Mental State Examination (HMMSE) by the same rater in a language of their choice (English, Sinhala, or Tamil), without repeating items common to both. The study was approved by the local institutional review board. Scales The HMMSE was created by amalgamating Folstein et al.'s MMSE [1] and Ganguli et al.'s Hindi Mental State Examination. [2] This was to improve its screening power without eliminating the MMSE's advantage of being not affected by education and culture fair as compared with the MMSE. The orientation items were as in the MMSE, but with minor modifications. Serial subtraction of 7s was replaced by serial subtraction of 3s. The unrelated words for learning and recall were administered in the same way as in the CONCOG. The repetition, visual comprehension, verbal sentence production, and copying items were as in the MMSE. This HMMSE is nearly identical to a previous Sinhala version of the MMSE validated in Sri Lanka. [3] The CONCOG is shown in the Appendix. It has items screening for the following cognitive domains: orientation to time (3 points), language (7 points), verbal episodic memory (8 points), visuospatial skills (4 points), and executive functions (8 points). We deliberately reduced the points for the orientation domain and allocated more weight to language, memory and executive function domains in keeping with their importance in the diagnosis of dementia and the differentiation of subtypes. The orientation item has only 3 points as compared with the MMSE which has 10 points. The language item includes naming of seven body parts. The memory item includes learning, delayed free recall, and multiple choice recognition of four unrelated words. Category verbal fluency (animals per minute) was chosen as the executive function item. The visuospatial domain includes copying of two simple diagrams (flower and diamond within a square). The total possible score on the CONCOG is also 30 in keeping with our aim of retaining the familiar format of the MMSE. Neuropsychological measures A subset of 30 patients also underwent neuropsychological assessment at the same time that the brief scales were administered. These neuropsychological measures consisted of
These tests assessed the domains of episodic memory, visual perception and spatial skills, praxis and executive functions. Statistics SPSS version 16.00 and MedCalc software [14] were used for all statistical analyses. Test-retest and inter-rater reliability for the CONCOG and correlations between the two scales and neuropsychological tests assessing the major cognitive domains were calculated using Kendall's coefficient b and Pearson's correlation coefficient. Multiple linear regression was employed to assess effects of age, gender, and education on test scores. Means, standard deviations, and percentile scores were calculated for groups stratified a priori according to age (≤75 and >75) and education (≤8 years and >8 years). One-way analysis of variance followed by post hoc comparisons using Scheffe's procedure were used to compare group differences. All analyses were two-tailed and the significance level was set at P<0.05. Results The total sample consisted of 204 subjects with a male:female distribution of 123:81. There were 58 subjects (28.4%) with less than five years of formal schooling and 15 (7.3%) with more than 15 years of education. There were 46 subjects (22.5%) over the age of 80 years and 12 (5.8%) below the age of 60 years. The CONCOG could be administered in less than 10 minutes and was well accepted by all subjects, as evidenced by no refusals. Internal consistency (Cronbach's alpha) for the CONCOG was 0.7. Inter-rater reliability was excellent (Kendall's tau-b=0.9). One month test-retest reliability was high (Kendall's tau-b=0.7). Of 204 subjects, only 12 subjects (5.7% of the sample) scored at ceiling level for the CONCOG compared with 30 (14.1% of the sample) for the HMMSE. The CONCOG also had a more normal distribution of scores than the HMMSE as shown in [Figure - 1]. Convergent validity was assessed by examining correlations (using Kendall's tau-b) between the CONCOG/HMMSE and neuropsychological measures of memory, praxis, visual perception and spatial skills, and executive functions to a subset of 30 subjects. The CONCOG showed significant correlations with neuropsychological measures of memory and executive function and better correlations with tests for perception and ideomotor praxis than the HMMSE [Table - 1]. Linear regression analyses to determine the influence of gender, age, and education on HMMSE and CONCOG test scores revealed the following: age and education, but not gender, significantly affected CONCOG and HMMSE test performances. Although the effect of age on both the scales was similar, the HMMSE was more affected by education than the CONCOG [Table - 2]. Correlations between the subtests of the CONCOG and age and education were also determined - education had significant positive correlations with all subtests except memory, whereas age had significant negative correlations with verbal fluency, memory, and copying subtests. We also looked at the relative difficulty of each subscale of the CONCOG in the present sample by calculating the percentage of the whole sample that scored at ceiling level. The verbal fluency subscale was the one with lowest percentage of subjects scoring at ceiling level, while the orientation subscale showed the most number of subjects scoring at ceiling level [Table - 3]. Means, standard deviations, 7 th , 10 th , and 25 th percentile scores on the HMMSE and CONCOG for the four groups identified a priori were calculated. One way analysis of variance followed by post hoc group comparisons using Scheffe's procedure showed that the mean CONCOG and HMMSE scores were significantly different only for the following groups: group with age ≤75 and education >8 years vs. all other subgroups [Table - 4]. Discussion Our initial expectations in developing the CONCOG seem to have been met to a great extent. The new scale is brief, simple, and does not require any specialized test material. It has showed good construct validity, high test-retest and inter-rater reliability. It demonstrates significant correlations with neuropsychological measures of memory and executive functions and better correlations with tests for perception and ideomotor praxis than the HMMSE. Compared with the version of the MMSE used in this study, the new scale is less influenced by the level of education. It has also demonstrated less ceiling effects than the HMMSE. But unlike the MMSE, it samples all major cognitive domains, especially executive function tests, which is a very important domain in dementia screening especially for the subcortical dementias. Because the language and visuospatial items are also better represented, the CONCOG would also be useful in tracking the longitudinal progression of cognitive deficits in dementia. The memory subscale comprising four word learning followed by delayed free recall and recognition and the verbal fluency subscale would also prove to be useful in screening for subcortical dementias, where the memory impairment is of the retrieval type rather than one of storage. The reduced weighting given to the orientation subscale would help minimize false positive results, as has already been shown in a previous study from India. [10] Thus the CONCOG seems to perform adequately on five of the six psychometric measures recommended for an ideal dementia screening test. [15] We decided against the practice of choosing a well-established screening test and suitably adapt and translate that to meet our needs, [2],[3],[4] as we strongly believe that a screening test introduced in a language and socio-cultural milieu vastly different from the one in which it is intended to be used might not perform well as a test that has been primarily designed for use in that population itself. This might be so not only because of the varying educational levels in populations, but also due to differing importance given to various items that constitute these tests. For example, South Asian elders would be specially disadvantaged in copying a three dimensional cube or tests of phonemic fluency. This has already been substantiated in a few studies that have directly compared performance on cognitive screening items between Asian and Caucasian elders. [16],[17],[18],[19],[20] Even the use of a common screening instrument initially developed for a population with low literacy levels does not obviate the effects of education and culture, as has been conclusively shown by the 10/66 dementia research group in the largest ever normative study of a cognitive screening test (Community screening instrument for dementia). [21] The MMSE (in a translated or adapted version) has been administered to elders in the Indian subcontinent in a few studies. [22],[23],[24] It has been directly compared with the Rowland Universal Dementia Assessment Scale (RUDAS) and the Addenbrooke's Cognitive Examination (ACE). A small pilot study assessed the equivalence between the MMSE and HMSE in a North Indian site, and concluded that there were discrepancies in classification of cognitive status using either scale. [23] In the largest such comparative study to date, it was shown that education and age significantly affected scores on the MMSE and ACE, with the level of education having a far greater influence on test scores than age. [22] Gender did not significantly affect scores in that study. In the study that compared the MMSE with the RUDAS, education had stronger correlation with the MMSE than the RUDAS. [24] Similar to the above studies, age and education, but not gender, were found to significantly affect scores on the Community Screening Interview for dementia (CSI-D) in both rural and urban Indian sites. [21] A few limitations to this study also need to be pointed out. The sample size of 205 is not adequate enough to develop norms for a cognitive screening test. The subjects recruited here might not be fully representative of elders living in the community with varying educational and socioeconomic levels. More robust norms for the scale can only be developed, if longitudinal follow-up of these normal elderly subjects is done and scores of those who subsequently go on to develop any cognitive impairment are excluded. In keeping with the recommendations of the Vascular Cognitive Impairment Harmonization standards committee the CONCOG fits into the role of a 5 minute screen. [25] However, the goals expected to be fulfilled with its development would be achieved only if we demonstrate that the CONCOG is sensitive enough to detect mild cognitive impairment. These studies are currently underway and would form the bases for future publications. [Appendix] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10193t4.jpg] [ni10193t1.jpg] [ni10193a1.jpg] [ni10193t2.jpg] [ni10193t3.jpg] [ni10193f1.jpg] |
| |||||||||


![[Figure - 1]](/showimage?ni/photo/ni10193f1.jpg){kind=link}
![[Table - 1]](/showimage?ni/photo/ni10193t1.jpg){kind=link}
![[Table - 2]](/showimage?ni/photo/ni10193t2.jpg){kind=link}
![[Table - 3]](/showimage?ni/photo/ni10193t3.jpg){kind=link}
![[Table - 4]](/showimage?ni/photo/ni10193t4.jpg){kind=link}
{kind=link}