 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
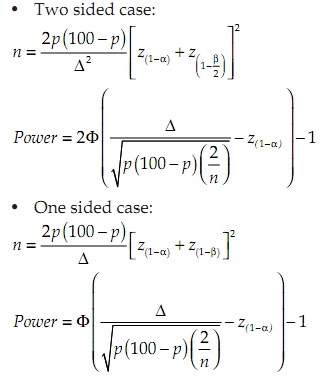
Neurology India, Vol. 58, No. 5, September-October, 2010, pp. 723-726 Topic of the Issue: Original Article Duration of anti-tubercular treatment in tuberculous meningitis: Challenges and opportunity Kameshwar Prasad, Jitendra Kumar Sahu Department of Neurology, All India Institute of Medical Sciences, New Delhi, India Correspondence Address: Date of Acceptance: 15-Oct-2010 Code Number: ni10197 PMID: 21045495 DOI: 10.4103/0028-3886.72182 Abstract Background: The duration of anti-tuberculous therapy in tuberculous meningitis is controversial. There is variation in recommendations by different societies and expert groups on this issue. Objective: To determine the strength of evidence for short-term therapy in tuberculous meningitis through review of literature and critical appraisal. Materials and Methods: Cochrane CENTRAL (Issue 4, 2010), TRIP database, and PubMed (from 1966 to present) were searched for relevant papers with keywords 'meningeal tuberculosis' and tuberculous meningitis' combined with 'chemotherapy'. A critical appraisal of a systematic review was done using standard criteria. Results: A total of 10 relevant papers were identified. All papers were included in a systematic review. The systematic review did not specify study design of studies to be included, had only case series but no randomised controlled trial, and unclear definition of endpoints. Conclusions: The evidence base for short-term therapy for tuberculous meningitis is weak. There is a need to conduct a randomised controlled trial with non-inferiority hypothesis of adequate sample size with well-defined end points and adequate follow-up. This is a challenge as well as opportunity for Indian neurologists. Keywords: Randomized controlled trial, short-term chemotherapy, systematic review, tuberculous meningitis Introduction Controversy surrounds the optimum regimen and duration of anti-tuberculous therapy in tuberculous meningitis (TBM). Various recommendations in literature include the following: WHO (2010) recommendations WHO Recommendation 1.1: It states that "New patients with pulmonary tuberculosis (TB) should receive a regimen containing 6 months of rifampicin: 2HRZE/4HR (Strong/High grade of evidence) Remark a: Recommendation 1.1 also applies to extrapulmonary TB except TB of the central nervous system (CNS), bone, or joint for which some expert groups suggest longer therapy (Chapter 8)." Chapter 8 states that "Pulmonary and extrapulmonary disease should be treated with the same regimens (Chapter 3).1 Note that some experts recommend 9-12 months of treatment for TB meningitis (2, 3), given the serious risk of disability and mortality. In TBM, ethambutol should be replaced by streptomycin."[1] British Infection Society (2009) recommendations "The recommended first-line treatment regimen for all forms of CNS tuberculosis is given in (A,II). Drugs should be taken each day either individually or in combination (B,II). Patients should be treated for a minimum of 12 months (A,II)." [2] Indian Academy of Pediatrics (2010) recommendations "In patients with TB meningitis on Category I treatment, the four drugs used during the intensive phase can either be HRZE or HRZS. The present evidence suggests that ethambutol can be used in children. Continuation phase of treatment in TB meningitis, miliary and spinal TB with neurological complications should be given for 6-7 months, extending the total duration of treatment to 8-9 months." [3] American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America (2003) recommendations "The basic principles that underlie the treatment of pulmonary TB also apply to extrapulmonary forms of the disease. Although relatively few studies have examined treatment of extrapulmonary TB, increasing evidence suggests that 6- to 9-month regimens that include isoniazid (INH) and rifampicin (RIF) are effective. Thus, a 6-month course of therapy is recommended for treating TB involving any site with the exception of the meninges, for which a 9- to 12-month regimen is recommended." [4] Furthermore, there is a plethora of recommendations in papers, talks, reviews, monographs, and textbooks explaining how long to use anti-tuberculous therapy, which are based on one's opinion rather than on evidence; not surprisingly, the recommendations are mutually conflicting, unclear, invalid, and unreliable. [5],[6] Many of these therapies have failed to persuade the medical community to adopt them. This article aims to examine the evidence base for such recommendations and highlight the need for and considerations for adding more evidence to the base. Materials and Methods We searched the following databases for relevant papers: PubMed, Cochrane CENTRAL (Issue 4, 2010), and TRIP database (assessed on October 2, 2010). The keywords used for searching were 'meningeal tuberculosis', tuberculous meningitis' combined with 'chemotherapy'. A paper often quoted to support a 6-month treatment of TBM is a systematic review by van Loenhout-Rooyackers et al.[7] We conducted a critical appraisal of the systematic review using the checklist of questions by Guyatt et al.[8] Results In literature search, we identified 10 papers regarding outcome of TBM in relation to the treatment duration. None of the studies had randomised controlled design. We did not find any paper published after the year 1998. All papers are case series published before 1999 and are summarised in a systematic review by van Loenhout-Rooyackers et al.[7] A critical appraisal of the systematic review reveals the following: Study design Authors mention explicit criteria for the studies to be included in the review, i.e. (1) the diagnosis of TBM was based on clinical findings, CSF analysis, and epidemiological data; (2) treatment included at least HRZ, possibly in combination with ethambutol and/or streptomycin in adequate doses; and (3) follow-up after treatment was at least 12 months. However, there is no mention of the study design in the list of criteria. Appropriate study design is a key criterion to allow selection of potentially valid studies in a systematic review. The study design most appropriate to compare short-term versus long-term treatment is a randomised controlled trial. It is clear that the authors did not find any randomised controlled trial to address this question. They found only case series of short-term (6 months) and long-term (> 6 months) treatment. Comparison between different case series is associated with high risk of bias. Specifically, the patients in the two groups may not be prognostically comparable, as is evident in this review (deaths during treatment were 16% in the short-term group versus 6% in the long-term group). Non-compliance is a well-established marker of patients' characteristics that favours poor prognosis, and this was also strikingly different in the two groups (2% in short-term group versus 10% in long-term groups). The best strategy to balance the known and unknown prognostic factors of patients between groups is randomisation that has not been used in comparing the two treatment durations. Losses to follow-up Authors identified relapse as the key outcome variable for comparing the two regimens, and also set a minimum of 12 months of follow-up after treatment. However, only 39 of 131 patients (30%) in short-term groups and 307 of 591 patients (52%) in the long-term groups completed the follow-up. Large number of losses to follow-up threatens the validity of any comparison. TBM affects patients of low socio-economic groups. Many patients do not come for follow-up after treatment completion because they lose their livelihood and shift to their parent villages or suffer relapse and take to some alternative form of treatment. Comparing only those who came for follow-up may yield erroneous results. Heterogeneity of case definitions The case definition of TBM varies in different studies. Culture positivity in the CSF also differs in the short-term and long-term treatment regimens (24% and 32%, respectively). Unclear definition of endpoints Authors mention on 'page 1031, last para' that all included studies did not mention the percentage of patients who were cured or those who were cured but had residual neurological deficits. The definition of these endpoints has not been given. The key outcome 'relapse' was not defined clearly in the review or in the included studies. This has resulted in confusing presentation of data from Goel et al. [9] who counted recurrence of symptoms due to non-compliance as 'relapse'. Language bias in selection of studies There is a language bias in selection of studies, as literature search was restricted to papers published in English language only. No attempt to limit reviewers' bias There is lack of attempt to minimise random error and systematic error in the selection of studies through independent selection by two reviewers at least. Having two or more people participate in each decision guards against errors; moreover, if there is good agreement beyond chance between the reviewers, the results would be more reliable. Discussion Our search clearly shows lack of randomised comparison between the short-term and long-term treatment of TBM. There is a clear need for a randomised controlled trial addressing this question. The following considerations may be important to consider when planning such a study. Clinical considerations Untreated TBM is highly fatal, which is recognised universally. In fact, many articles emphasise this feature of untreated TBM. Such a serious condition requires that the treatment given to patients is adequate, promotes survival, and does not lead to relapses. Thus, the endpoints, which are relevant for consideration of any change in treatment duration, are survival and frequency of relapses. While survival is easy to ascertain and is evident within 6-9 months of therapy, the relapses are likely to occur months or even years after inadequate treatment and requires a long follow-up to ascertain. Therefore, whether short-term treatment is as good as the long-term one, requires establishment of similar rates of case fatality and relapses. In studies, which aim to establish equivalence of short-term and long-term treatment, therefore need to have a follow-up of some years' duration-probably two years, and preferably 5-10 years. There are two points to consider: (i) the endpoints of a trial comparing short-term versus long-term treatment in TBM are binary (comparison of percentages of deaths or relapses); (ii) the follow-up of such a study needs to capture 'relapses' and therefore, needs to be of minimum two years, and preferably 5-10 years. Statistical considerations A common error in the assessment of a study comparing short-term and long-term treatment is that 'absence of proof of difference is taken as proof of absence of difference'. Here, one is not concerned with demonstrating that there is no statistically significant difference between short-term and long-term treatment. If this is so, one can easily take 20 patients (10 for short-term and 10 for long-term treatment), and thereby guarantee that there will be no statistically significant difference between the two arms. Rather, it is important to appreciate that the sample size formula [10] for the comparison of two treatment strategies has the following general formula:-
In this formula, Δ denotes the difference in percentage of success or failure rate. When one considers equivalence between two treatment regimens then one is essentially looking for D of zero, and zero in the denominator of any mathematical calculation would lead to infinity. Essentially, this means that exact equivalence between the two treatment regimens cannot be established. In order to avoid this situation, investigators decide an acceptable level of inferiority margin and attempt to show that the difference between the two treatment regimens does not exceed the level of inferiority margin that they consider as acceptable. Therefore, a more common terminology used for such trials is non-inferiority trial rather than equivalence trial (though some investigators consider both as the same, while others consider equivalence as a two-sided case and non-inferiority as one-sided case). Thus, the only option for investigators comparing short-term and long-term regimens is to carry out a non-inferiority trial with a pre-specified level of acceptable inferiority margin. The question is what level of inferiority margin is acceptable? In other words, how much difference in outcome between two treatment regimens may be ignored? [Table - 1] gives the sample size for different levels of inferiority margin (i.e., difference to be ignored). [Table - 1] explains clearly that the sample size required in a study comparing short-term versus long-term regimen needs to be multi-centric to have adequate sample size, within an acceptable time frame. Another important statistical consideration in the non-inferiority trial is that intention-to-treat analysis may be misleading. Details are beyond the scope of this paper (interested readers may read paper by Jones B et al. [10] ). It is sufficient here to say that both intention-to-treat and pre-protocol analysis need to show equivalent results to be convincing. One can conclude that the most reliable and valid method to find out the most appropriate duration of anti-tuberculous therapy is to conduct a multicentric randomised controlled trial. Unfortunately, this critical issue has not been examined in a randomised trial. This is ironical in the sense that streptomycin in TB was one of the first interventions in medicine to be subjected to a randomised trial. With large number of cases and availability of required facilities and expertise, India is probably the most appropriate place to conduct such a trial. This is an opportunity that neurology community in India must seize. Abbreviations HRZE: Isoniazid+rifampicin+pyrazinamide+ethambutol HR: Isoniazid+rifampicin References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10197t1.jpg] |
| |||||||||

![[Table - 1]](/showimage?ni/photo/ni10197t1.jpg){kind=link}