 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
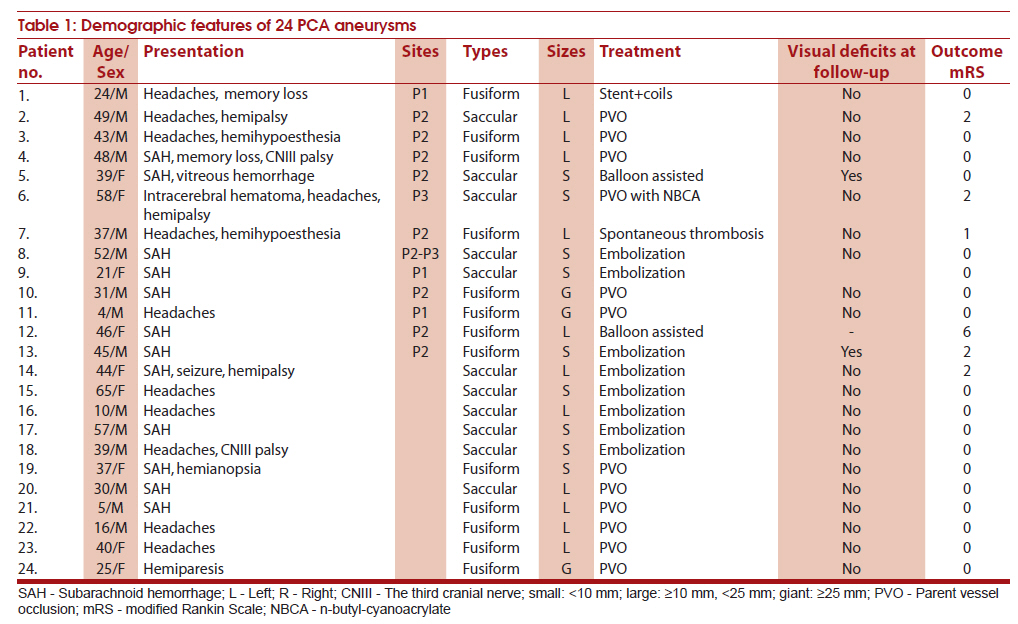
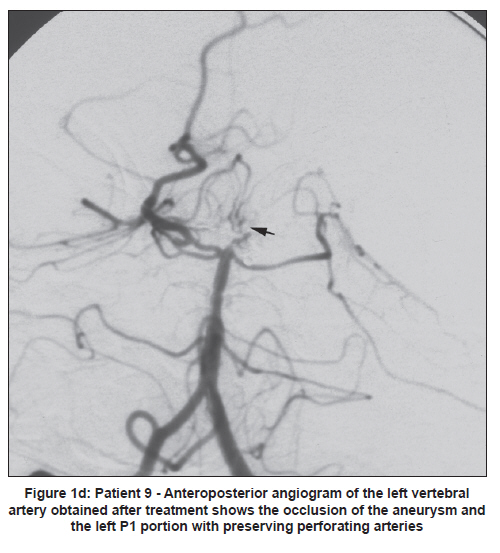
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 6-11 Original Article Characteristics and endovascular treatment of aneurysms of posterior cerebral artery Jian Wang1, Zhigang Sun2, Jinsuo Bao1, Bin Zhang1, Yan Jiang1, Wenjing Lan3 1 The Affiliated Hospital of Inner Mongolia National University, Tongliao, Inner Mongolia, China Date of Submission: 04-Jan-2010 Code Number: ni11003 PMID: 21339651 Abstract Background : Aneurysms of the posterior cerebral artery (PCA) are a distinct rarity and present with some peculiar morphologic features and specific clinical findings. These aneurysms can be managed endovascularly with good results.Objective : To evaluate the clinical features and endovascular management of PCA aneurysms. Material and Methods : Between 2000 and 2008, we treated 24 patients (14 male and 10 female; mean age: 36 years) with PCA aneurysms. Clinical presentations, radiologic images, and endovascular management were reviewed. Results : There were 11 saccular aneurysms, including 4 giant or large aneurysms, and 13 dissecting aneurysms, including 11 giant or large aneurysms. Of the 24 patients, 13 presented with hemorrhage and 6 with neurologic deficits. Five patients presented with headaches without any neurologic deficits. Parent vessel occlusion was performed in 12 patients, selective coil embolization was performed in 11 patients, and 1 patient conservatively. Eighteen patients had a good recovery, 5 had a moderate disability (one with 1 visual deficit after the treatment) related to hemorrhage, vasospasm, or infarction before aneurysm trapping, and 1 patient died because of rebleeding. The conservatively treated patient made a good recovery. Conclusion : PCA aneurysms have specific clinical characteristics compared with aneurysms located elsewhere. Endovascular technique can achieve good outcomes despite the aneurysmal site and size. Keywords: Aneurysm, endovascular therapy, posterior cerebral artery Introduction Aneurysms of the posterior cerebral artery (PCA) are a distinct rarity with an incidence of 0.7%-2.3%. [1],[2],[3],[4] Nevertheless, they have been recognized as an important cause of bleeding. These aneurysms have some peculiar morphologic features and present with specific clinical findings that distinguish them from aneurysms occurring at other anatomic locations of cerebral circulation. [3],[5] Aneurysms of the PCA are also an important cause of stroke in younger patients. [4],[6] Also, there is a higher incidence of large and giant aneurysms. Compared with aneurysms located elsewhere, the site, size, and surgical techniques used do not significantly affect the prognosis of patients with PCA aneurysms, because, unlike aneurysms at other sites, there is rich collateral flow in areas fed by the PCA. [7],[8] However, recent data confirm good results when these aneurysms are treated by endovascular techniques. [4],[6],[9],[10],[11],[12],[13] We review our 8-year experience with these relatively rare aneurysms involving the PCA and discuss the specific clinical characteristics and endovascular management used to treat PCA aneurysms. Material and Methods During the 8-year period from 2000 to 2008, of the 1956 patients with aneurysms seen at Beijing Tiantan Hospital, 24 patients (1.2%) were with PCA aneurysms, 14 men and 10 women, in the age range from 4 to 65 years (mean, 36 years) [Table - 1]. Diagnosis was based on clinical presentations and radiologic findings, including computed tomography (CT) scanning, magnetic resonance imaging (MRI), and cerebral angiography. Intramural thrombus on T1-weighted images and intimal flaps on T2-weighted images were the major findings indicating dissecting aneurysm. All the patients underwent cerebral digital subtraction angiography (DSA), which demonstrated such typical results as double lumen, tapered narrowing, or occlusion with or without aneurysm dilation, and retention of contrast medium. A sequential change in luminal configuration also supported a diagnosis of dissection. Of the 24 aneurysms, 11 were saccular, including 4 giant or large aneurysms, and 13 were dissecting aneurysms, including 11 giant or large aneurysms. Of the 24 patients, subarachnoid hemorrhage (SAH) was the presenting feature in 12 and cerebral hemorrhage in 1 patient. Six patients presented with neurologic deficits and 5 with headache without any neurologic deficits. In 1 patient, SAH due to rupture of aneurysm at another site, was an incidental finding. The Hunt and Hess grade at admission was grade 0: 10; grade 1: 10; grade 2: 3; and grade 3: 1. Each segment of the PCA was classified according to the classification of Kaweshima and Rhoton. [8] The aneurysm location was P1 segment in 5 patients, P2 segment in 17 patients, P2-P3 junction in 1 patient, and P3 segment in 1 patient. The outcome was assessed using modified Rankin Scale (mRS). Treatment strategies Our basic treatment strategy for PCA aneurysms was endovascular. Early embolization within 48 h after SAH was performed in 1 patient with Hunt and Hess grade 1 and the remaining patients underwent delayed embolization.
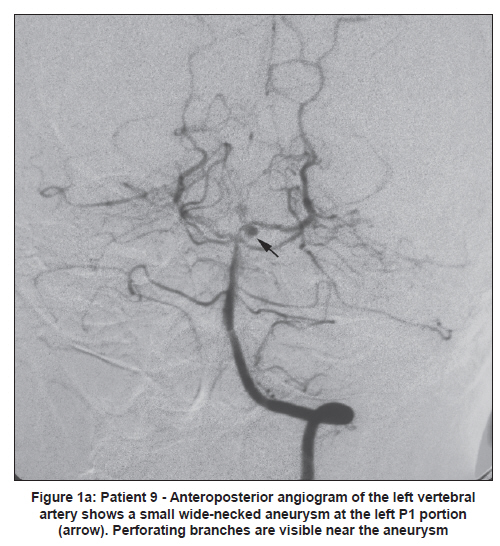
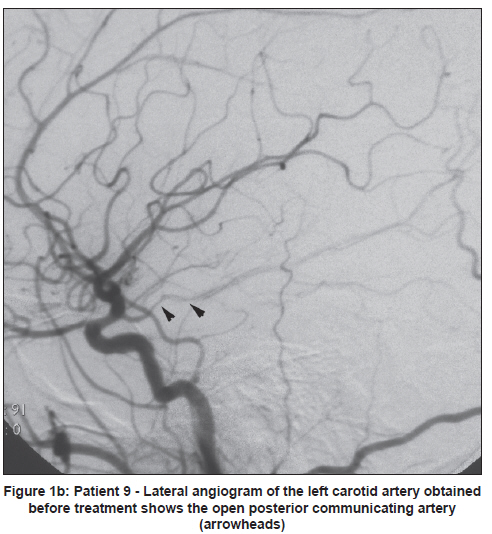
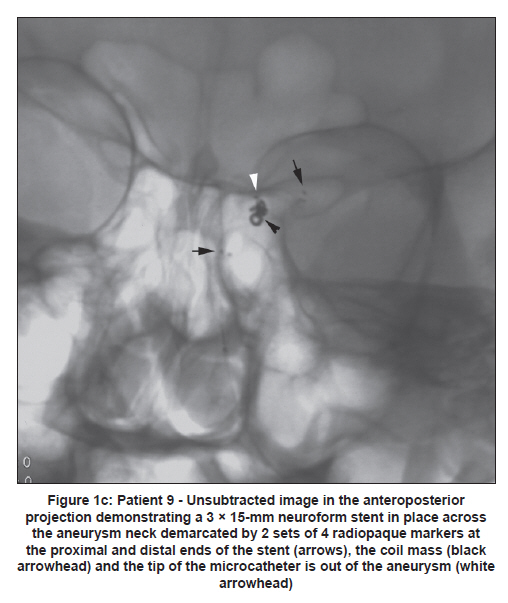
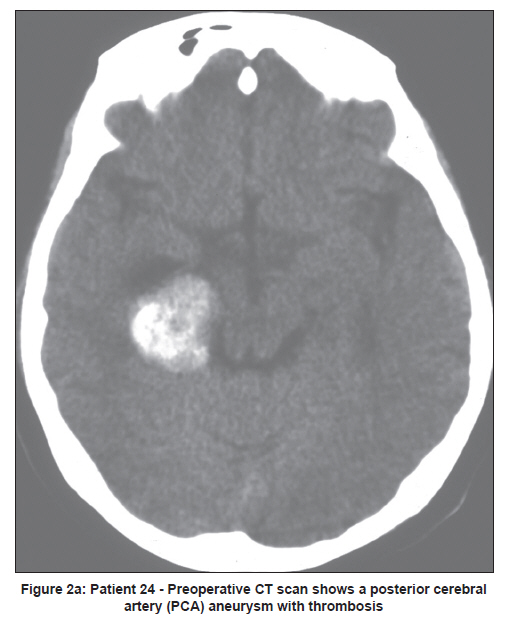
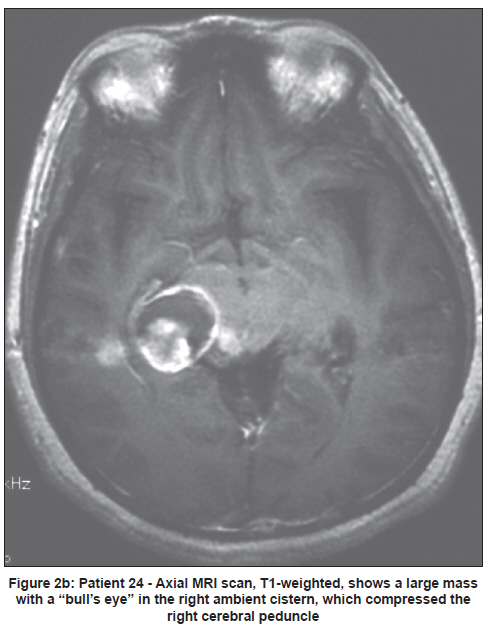
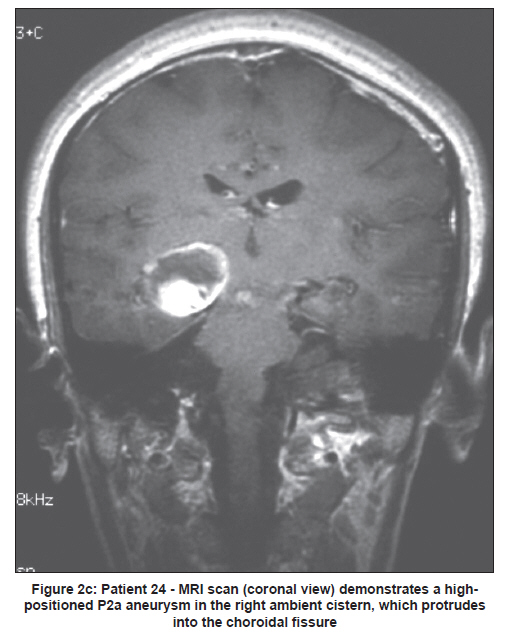
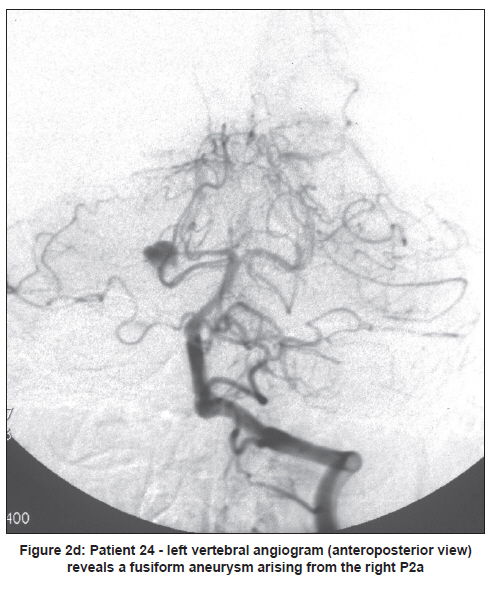
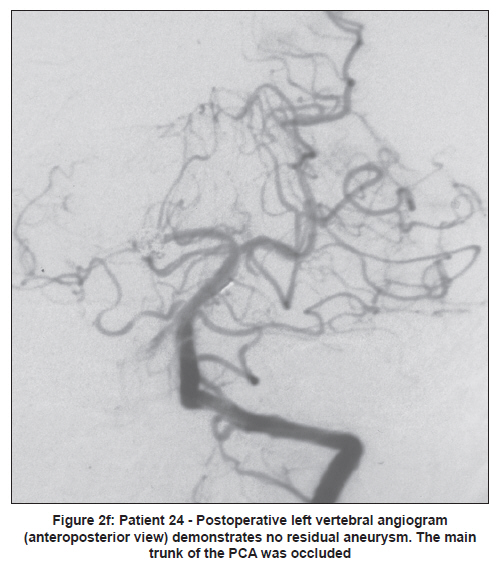
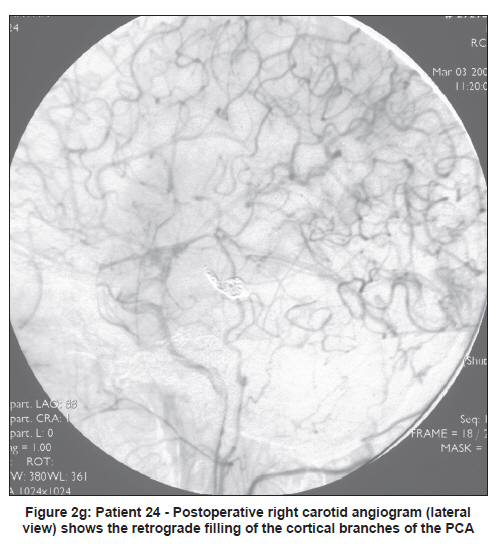
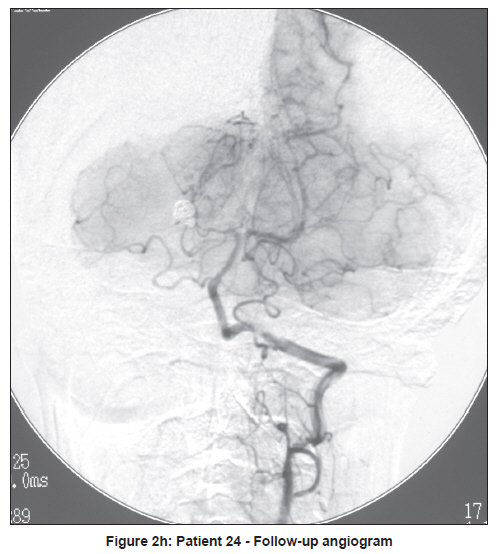
Outcomes Of the 24 patients, 18 (75%) made a good recovery (mRS = 0) and 5 had a moderate disability (mRS = 1-2) related to hemorrhage, vasospasm, or infarction. The patient who was managed conservatively had spontaneous thrombosis of aneurysm and made a good recovery. There was one death among the patients with ruptured aneurysms because of incomplete embolization and rebleeding. Of the 12 patients who underwent PCA sacrifice, the patients who underwent parent vessel occlusion demonstrated no homonymous hemianopsia. Illustrative cases Case 9 A 21-year-old woman was admitted on the previous day at another hospital for SAH. At admission she was alert with no neurologic deficit. DSA revealed a small broad-neck saccular aneurysm in the P1 segment of the left PCA [Figure - 1a]. She was transferred to our hospital for further evaluation and treatment [Figure - 1a, Figure - 1b, Figure - 1c and Figure -1d]. On the next day, stent-coil embolization was performed and her postoperative course was uneventful. She was neurologically intact at 3 months of follow-up. Case 24 A 25-year-old woman underwent CT for acute onset of left hemiparesis, which revealed a mass lesion measuring 30 mm in diameter compressing the right cerebral peduncle [Figure - 2a, Figure - 2b, Figure - 2c]. Cerebral angiography revealed a dissecting aneurysm at the right P2a segment [Figure - 2d]. The aneurysm was treated with parent vessel occlusion. At 6-month follow-up, the patient showed no neurologic deficits [Figure - 2f, Figure - 2g, Figure - 2h]. Discussion Aneurysms arising from the PCA frequently affect young patients. [12] The average age in our series was 36 years, a much younger age than the patients (range, 50-60 years) with aneurysms at other anatomic sites. PCA aneruysms tend to be large or giant dissecting aneurysms. [3] In our series, of the 24 aneurysms, 15 (62.5%) were either large or giant, a higher frequency than frequently reported by others. The location of aneurysms at various segments of PCA in our series was similar to the reported findings in other series. [1],[3],[4],[6],[11],[12] The frequently found location was P2 segment. The most common clinical presentation of PCA aneurysms is SAH as seen in our series. The overall morbidity and mortality in our series was 25%, similar to the morbidity and mortality seen in patients treated for aneurysms in the anterior circulation at our hospital. The reported rates of homonymous hemianopia following proximal P2 occlusion varied between 4.5% and 14%. [12] There were few associated vascular anomalies in our series: basilar fenestration and multiple intracranial aneurysms in one patient each. One of our patients had spontaneous thrombosis of the aneurysm. However, the natural history of thrombosed intracranial aneurysms is not well studied. Although our patient was neurologically stable at 2-year follow-up, we suggest long-term follow-up of such patients to define the natural history. Endovascular surgery is associated with good results in aneurysms of the posterior circulation, including the PCA. [14] Aneurysms in the P2 segment are well suited for parent vessel occlusion with detachable coils because the perforating branches are close to the cerebral peduncle. [11],[12],[15] We obliterated 2 small saccular aneurysms with coils and embolized 1 aneurysm arising from the branch of P3 segment with liquid material. We found that endovascular obliteration using coils is safe and effective in cases with small PCA aneurysms with a small neck. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11003f2d.jpg] [ni11003f2b.jpg] [ni11003f2c.jpg] [ni11003f2e.jpg] [ni11003t1.jpg] [ni11003f2h.jpg] [ni11003f2g.jpg] [ni11003f1b.jpg] [ni11003f1c.jpg] [ni11003f2a.jpg] [ni11003f1d.jpg] [ni11003f2f.jpg] [ni11003f1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}