 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
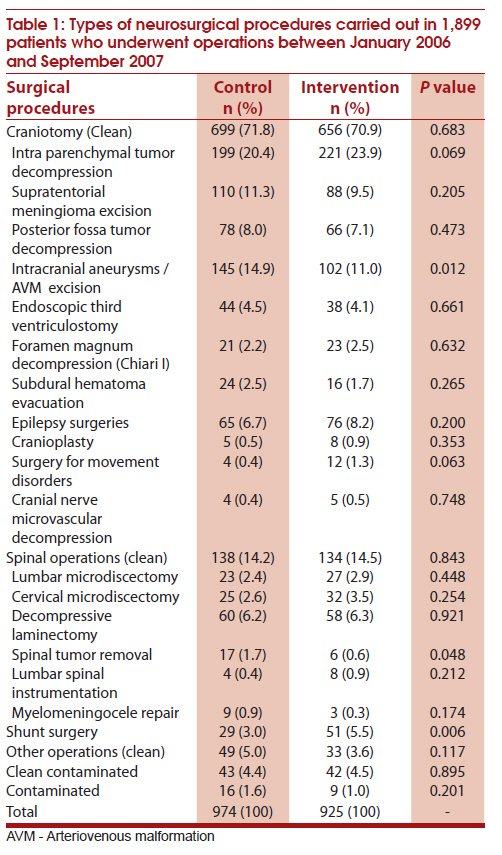
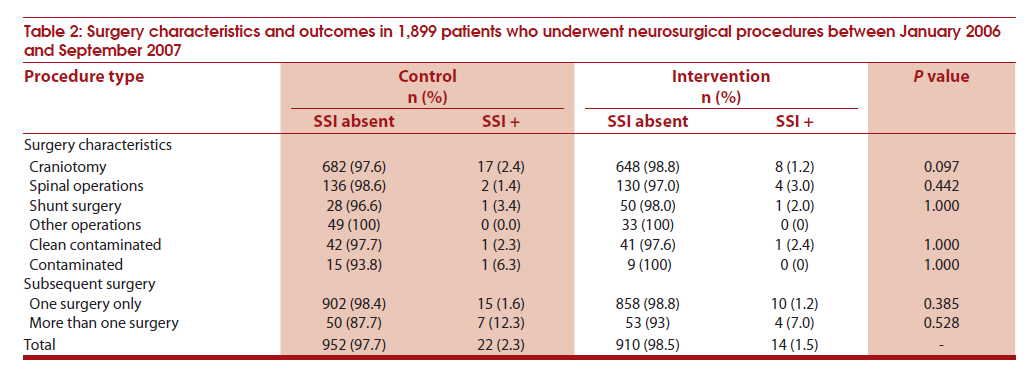
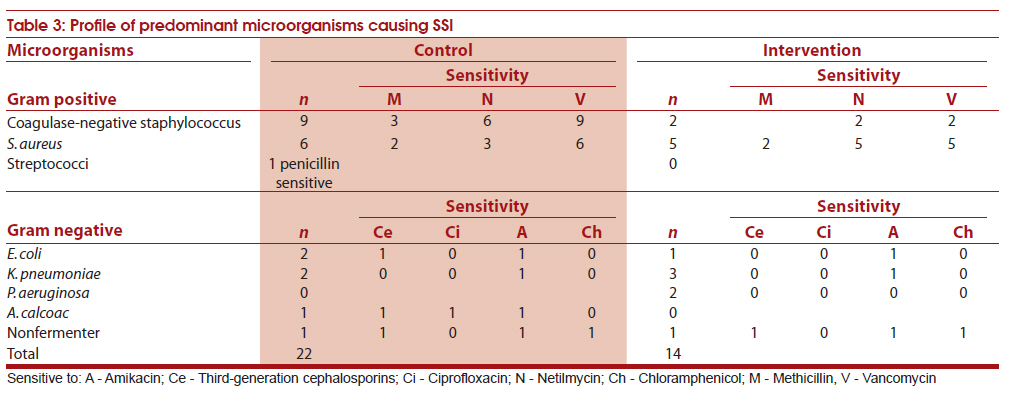
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 12-17 Original Article Alcohol-based hand rub and surgical site infection after elective neurosurgery: An intervention PP Saramma1, K Krishnakumar2, PS Sarma3 1 Division of Nursing Education, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala, India Aim : To evaluate the effect of alcohol-based hand rub before and after each patient contact on SSI after elective neurosurgical procedures. Setting and Design : Department of Neurosurgery, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala. An intervention study using a 'before-after' design. Material and Methods : Two 9-month study periods were compared; between these periods, an infection-control protocol incorporating an alcohol-based hand rub was implemented for a period of 3 months and continued thereafter. Consecutive patients who underwent neurosurgery between January and September 2006 (control group, before protocol) and between January and September 2007 (intervention group, after protocol) were included. Outcome measures included SSI rates, profile of microorganisms and patient survival. Statistical Analysis : SPSS statistics version 17.0. Results : A total of 1,899 operated cases were reviewed. The patients in the control and intervention groups were similar with regard to sex, age and type of neurosurgery. The surgical site infection rates were 22 (2.3%) out of 974 in the control group and 14 (1.5%) out of 925 in the intervention group (P = 0.2). Patient survival rates were 97.6% (control) and 98.3% (intervention). Post hoc power calculation for an alpha value equal to 0.05, the power obtained was 24.9%, showing inadequacy of sample size to get significant results. To achieve 80% power, the sample size required is about 4,800 each for the control and intervention groups. Conclusion : Use of alcohol-based hand rub before and after each patient contact in the neurosurgical intensive care unit did not show a significant reduction in SSI in the present study. This lack of difference between the two groups may be related to the inadequate sample size. The other possibility is that both the strategies are of equal efficacy for prevention of SSIs. Keywords: Alcohol-based hand rub, hand hygiene, neurosurgical, surgical site infection Introduction Surgical site infection (SSI) accounts for approximately a quarter of all nosocomial infections. [1] The risk of developing an SSI is associated with a number of factors, including surgical, patient and microbial characteristics. [2] Each SSI is associated with approximately 7 to 10 additional postoperative hospital days. [3],[4] It is estimated that 77% of deaths among patients with SSI are directly attributable to SSI. [5] Postoperative neurosurgical infections have high morbidity rates and are among the most life-threatening infections. [6] Hand hygiene is promoted as the most effective means of preventing healthcare-associated infections (HAIs). Hand rubs may be an alternative to hand washing [7] and are the first choice according to the World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) guidelines. Studies have shown that an alcohol-based antiseptic rub decontaminates hands effectively for a wide variety of organisms. [8],[9] We implemented the use of alcohol-based hand rub before and after each patient contact in the neurosurgical intensive care unit and undertook a study to analyze the types of SSIs before and after the implementation of the use of alcohol-based hand rub, after elective neurosurgical procedures. Material and Methods Setting This study was undertaken in the department of neurosurgery of a tertiary-level referral hospital in Kerala, India. This institute is a 239-bedded hospital for tertiary care of cardiovascular and neurological diseases. The department of neurosurgery has a bed strength of 50, including a 13-bedded intensive care unit. More than 1,400 surgical admissions and 1,300 elective adult and pediatric neurosurgical procedures are performed every year. Specific infection-control protocols followed in this department include treating remote infection before elective operation, restricting shaving of hair to early morning of the day of surgery, controlling serum blood glucose perioperatively, and giving antiseptic shower the night before and the morning of an elective operation. Usually patients are transferred to the neurosurgical ward on the first or second postoperative day and are discharged within 7 to 9 days. All the patients received antibiotic prophylaxis during the study period. Usually intravenous chloramphenicol/ceftriaxone and amikacin are given from the previous night of surgery and discontinued on the second postoperative day. There was no antibiotic policy change during the study period. In this department, health care workers used soap and water for maintaining hand hygiene, and the use of alcohol-based hand rub was limited to decontaminating hands before invasive procedures. The infection control nurse (ICN) of the institute maintained the concurrent record of health care-associated infections, including SSIs. The ICN collected the data by direct method of surveillance during surgical admission of these patients and also covered 1-month follow-up visits. Department of microbiology undertook bacterial culture and sensitivity of the organisms to 50 different anti-infective agents. The antibiotic sensitivity of gram-positive organisms for the entire institute for the month of January 2006 was: amikacin (68%), gentamicin (43%), penicillin (57%), Cloxacillin (72%), cephalothin (21%) and vancomycin (100%). The antibiotic sensitivity of gram-negative organisms during the same month was: amikacin (69%), gentamicin (35%), tobramycin (40%), ceftriaxone (25%), cefperazone+sulbactum (40%), ceftazidine (22%), ciprofloxacin (32%), ofloxacin (52%), netilmycin (67%) and chloramphenicol (56%). Types of neurosurgical procedures Neurosurgical procedures were classified into four categories based on the wound type: 'clean,' 'clean contaminated,' 'contaminated,' and 'dirty.' [10] The 'clean' cases included all elective neurosurgical procedures in which no inflammation was encountered and neither respiratory nor alimentary tract is entered (clean craniotomies, spinal surgeries); 'clean contaminated' cases included cases with known risk factors such as entry of paranasal sinuses/ respiratory tract/ alimentary tract under controlled conditions like transnasal transsphenoidal procedures, and transoral procedures; and 'contaminated' and 'dirty' cases included surgical sites in which acute nonpurulent inflammation was encountered and / or neurosurgeries where pus was encountered during the operation or sepsis was present at the time of surgery (cases with cerebrospinal fluid [CSF] leak, surgery for brain abscess, bone flap removal for osteomyelitis, and wound resuturing). Ventriculoperitoneal shunts were considered as a separate class, and surgeries under local anesthesia were included under other clean procedures. Infection-control protocol implementation We inculcated the habit of using alcohol-based hand rub before and after each patient contact among the health care workers. Chlorhexidine/alcohol skin antiseptic with emollient and moisturizer was made available at each bedside by having a permanent holding device for the hand rub in each patient unit. Hand hygiene-promoting posters were displayed in different areas in the unit, including the hand washing area. The use of alcohol-based hand rub was reinforced as an adjunct to washing the hands with soap and water. Formal hand washing with soap and water was done whenever there was visible soiling of hands. In addition, all the health care workers used the alcohol-based hand rub before and after each patient contact. A team consisting of the hospital infection-control nurse, the senior nursing staff and one neurosurgeon took the responsibility for ensuring that hand hygiene became a habit among all health care workers. This was achieved through regular in-service training to all health care workers. The implementation phase extended from October 2006 to December 2006. SSI definitions The criteria of the CDC, [11] for SSI include the presence of any one of the following: a purulent discharge from the wound, a serous discharge with positive bacterial culture, a deep or superficial wound abscess with or without positive bacterial culture, wound swelling and erythema with or without pyrexia, or meningitis/ ventriculitis with positive bacterial culture or microorganisms seen on the G ram's stain, occurring within 30 days of the surgical procedure. In this study, an SSI was defined as having a discharge from the surgical site with a positive bacterial culture, or signs of meningitis with or without a positive CSF culture. Design and duration An interventional study (before-after design) was undertaken. The duration of the study extended from January 1, 2006 to September 30, 2007, excluding the protocol implementation period from October to December 2006. Sample The patients in the control group included consecutive patients who had undergone neurosurgery in the period from January 1, 2006 to September 30, 2006 before protocol implementation (control group, n = 974). The patients in the intervention group included consecutive patients who had undergone neurosurgery in the period from January 1, 2007 to September 30, 2007 after protocol implementation (intervention group, n = 925). In the present study, we excluded patients who had undergone neurosurgery during the transition period of protocol implementation (October 2006 to December 2006). A total of 1,899 patients had undergone 2,025 neurosurgical operations during the study period. The follow-up period for diagnosing SSI was at least 30 days for both the groups. Data collection The operating-theatre registers of the department of neurosurgery covering the study period were reviewed for getting the patients' details (age, sex, diagnosis, type of surgical intervention, and evidence of subsequent surgery). An indirect method of SSI surveillance, which included a detailed review of wound culture and sensitivity reports covering the study period and extending to 30 days, was undertaken. The surgical site culture and sensitivity reports of all these patients were reviewed from the records of the department of microbiology, covering the study period and for an extended period of 30 days to detect 30-day SSI. Health care-associated infection data maintained by the infection control nurse were reviewed to include patients with clinical signs of SSI as defined earlier. The medical records of patients with SSI were counterchecked and verified. Computer data on mortality from the Medical Records Department also were collected. Data analysis Data were analyzed using SPSS statistics version 17.0. The t test, chi-square tests or Fisher exact tests were done where appropriate; to assess statistical significance. Probability value of .05 or less was the criterion used to conclude statistical significance. Results The age of the control group ranged from 3 months to 81 years, with a mean of 38.45 ± 17.68 years; and that of the intervention group ranged from 3 months to 82 years, with a mean of 37.62 ± 17.1 years (P = 0.297). Children aged below 12 years accounted for 10.2% and 8.9% of the control and intervention groups, respectively (P = 0.335). Male predominance was noticed among both the groups (55% and 53.6%; P = 0.509). [Table - 1] lists the types of neurosurgical procedures in both the groups. The study groups were similar with regard to the types of surgical procedures except that there were more of intracranial aneurysms / AVM excisions (P = 0.012) and spinal tumor removals (P = 0.048) and less of shunt surgeries (P = 0.006) in the control group. The surgery characteristics and outcomes based on the presence of SSI are shown in [Table - 2]. The main outcome measure in this study was the effect of alcohol-based hand rub on SSI. SSIs were documented in 22 patients in the control group and 14 patients in the intervention group. Eight patients in the control group and 6 patients in the intervention group had postoperative meningitis. Among these patients, 3 each in both groups had postoperative CSF leak. The remaining patients, 14 in the control group and 8 in the intervention group, had superficial SSIs. The SSI rates were 22 (2.3%) out of 974 in the control group and 14 (1.5%) out of 925 in the intervention group. Though there was a reduction in SSI in the intervention group, it was not significant (P = 0.2). The incidence of SSI in clean procedures was higher for spinal operations (2.2%) than for cranial operations, (1.8%). Out of the 6 SSIs among the spinal operations, 5 were among patients who had undergone decompressive laminectomy. Fifty-seven patients each in the control group (5.8%) and intervention group (6.1%) had undergone subsequent surgeries during the study period. The number of subsequent neurosurgical procedures was 66 among the control group and 60 among the intervention group. When we analyzed the patients who had undergone more than one surgery, the rate of SSIs among them was higher (9.7%) than in patients who had undergone only one surgery (1.4%) . The SSI rate in the intervention group was lesser than in the control group in patients who had undergone only one surgery (1.2% and 1.6%, respectively), as well as in those who had undergone more than one surgery (7% and 12.3%, respectively). However, the differences were not significant (P=.385). Death rate due to neurological or other complications was 1.7% and 2.4% among the intervention group and the control group, respectively. One out of the 16 patients who died among the intervention group and 3 out of the 23 patients who died among the control group had SSIs, but none of these terminal events were attributed to SSI. Power analysis In order to provide a context for interpreting the accuracy of the nonsignificant results, a post hoc power calculation was done based on the sample size used in this study and the difference in proportion obtained. For an alpha value equal to 0.05, the power obtained was 24.9%, showing inadequacy of sample size to get significant results. To achieve 80% power, the sample size required is about 4,800 each for the control and intervention groups. Profile of microorganisms Profile of predominant microorganisms isolated from the wound/ CSF is given in [Table - 3]. The predominant microorganism isolated in patients with SSI in the control group was coagulase-negative staphylococcus. The predominant gram-negative microorganisms isolated among the intervention group were Klebsiella and Pseudomonas. Klebsiella organisms in both groups were extended-spectrum beta lactamase (ESBL) resistant. None of the infections were lethal, and the wounds healed after specific antibiotic therapy. Discussion The present study showed a reduction in the rate of surgical site infection among elective neurosurgical patients after the protocol implementation of alcohol-based hand rub, from 2.3% to 1.5%. To be specific, the reduction in incidence of SSI caused by coagulase-negative staphylococcus was observed, while gram negatives seemed to increase in the intervention group. The most common organisms isolated were coagulase-negative Staphylococcus, Staphylococcus aureus. Similar were the results in the earlier studies. [12],[13] Moralejo and Andrew [8] found that hand rubbing with an alcohol-based solution reduced bacterial contamination of health care workers' (HCWs' ) hands more than did hand washing with antiseptic soaps during routine patient care activities. Introduction of alcohol/ chlorhexidine hand hygiene solution (ACHRS) and a detailed culture-change program were effective in improving hand hygiene compliance and reducing nosocomial methicillin resistant staphylococcus aureus (MRSA ) infections. [9] The present study did not attempt to compare the effect of different hand-washing materials or techniques. However, a minimal decrease in the incidence of infection with MRSA and a minimal increase in the incidence of other gram-negative organisms were observed in the intervention group in the present study. Le et al. [14] prospectively demonstrated that the introduction of an alcohol-based hand sanitizer could reduce SSI rates in neurosurgical patients (with particular impact on superficial SSIs) and also reduce the overall postoperative length of stay and the duration of antimicrobial use. The results of the present study support the former part of the findings, especially the reduction in rates of SSIs caused by coagulase-negative staphylococci. Though the postoperative length of stay and the duration of antimicrobial use were not included in the present study, the observed reduction in SSIs indirectly supports the findings related to these observations. The overall incidence of SSI (1.9%) observed in the present study was well below the published data on SSI rate, 2.5-6.6% in patients undergoing neurosurgery/ craniotomy. [12],[13],[15],[16] This may be related partially to the elective nature of the neurosurgical procedures in this study. The achieved rate of SSI in clean craniotomies and shunt operations in the intervention group is comparable to the published rate of SSI in elective clean craniotomies and shunt surgeries. [6] However, the incidence of SSIs in clean procedures was higher for spinal surgery than for cranial surgery in this study. Valentini et al. reported a lower infection rate for spinal surgery than for cranial surgery. [6] The present series had higher percentage of decompressive laminectomies, procedures with long duration. Five out of the six SSIs among the spinal surgeries occurred in this category. It is well known that the SSI risk increases with duration of surgery. [6] This could be the reason for the observed higher infection rate in spinal surgery in this series. Postoperative cerebrospinal fluid leakage is the most important independent risk factor for SSI. [13],[16],[17] In the present study, 6 (43%) out of 14 patients who developed postoperative meningitis had CSF leak. Subsequent surgery is another independent risk factor for SSI. [13],[17] The present study also supports this. Though we could not find a difference in SSI rate between intervention and control subjects within a given group (one surgery or > one surgery), when both intervention and control groups were pooled together, one-surgery group had lower infection rates than the group which underwent multiple surgeries. However, after the introduction of alcohol-based hand rub, there was only a nonsignificant reduction in SSI rates in neurosurgical patients. In this study the introduction of use of alcohol-based hand rub before and after each patient contact in the neurosurgical intensive care unit did not show a statistically significant reduction in the SSI rates. The SSI rate in the control group also was very low, perhaps due to adherence to the then existing infection-control measures. This lack of difference in the SSIs with the introduction of use of alcohol-based hand rub may be related to the sample size in our study. Post hoc power calculation for an alpha value equal to 0.05, the power obtained was 24.9%, showing inadequacy of sample size to get significant results. To achieve 80% power, the sample size required is about 4,800 each for the control and intervention groups. Considering the clinical relevance of reduction in SSI, further large-sample studies are indicated to confirm the utility of the intervention. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11004t2.jpg] [ni11004t1.jpg] [ni11004t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}