 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
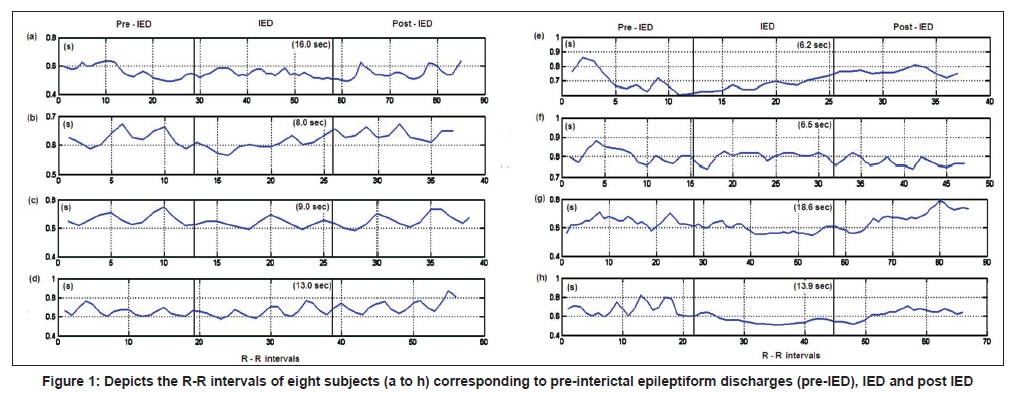
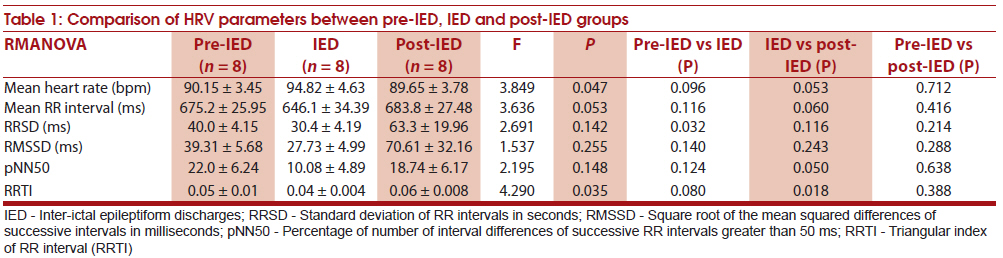
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 25-29 Original Article Quantitative analysis of heart rate variability in patients with absence epilepsy C Pradhan1, S Sinha1, K Thennarasu2, T Jagadisha3 1 Department of Neurology, National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, India Date of Submission: 27-Jul-2010 Code Number: ni11006 PMID: 21339654 Abstract Background : There are no studies quantifying the nature of autonomic changes in absence epilepsy.Aims : We characterized the heart rate variability (HRV) during pre-interictal epileptiform discharges (IED), IED and post-IED states in absence epilepsy. Material and Methods : Electroencephalogram (EEG) records with generalized 3-Hz spike-wave discharges in 8 patients (M: F: 3 : 5; mean age: 13.0 ± 2.5 years) with absence epilepsy were identified and corresponding electrocardiogram (ECG) time series were obtained. The time domain HRV measures were applied to pre-IED, IED and post-IED simultaneous ECG tracing. Results : There was slight tachycardia during the IED phase (pre-IED: 90.15 ± 3.45 bpm, IED: 94.82 ± 4.63 bpm, P = 0.09) which returned to baseline during the post-IED phase (post-IED: 89.65 ± 3.78 bpm). There was significant decrease in the standard deviation of RR interval (pre-IED: 40.0 ± 4.15 ms, IED: 30.4 ± 4.19 ms, P = 0.032) and trend in reduction of triangular index (pre-IED: 0.05 ± 0.01, IED: 0.04 ± 0.004, P = 0.08) during the IED phase when compared to pre-IED phase. The percentage of RR intervals >50 ms was lower during the IED phase and achieved significance when compared to post-IED phase (IED: 10.08 ± 4.89, post-IED: 18.74 ± 6.17, P = 0.050). While mean HR and RR interval significantly correlated with the duration of IEDs, there was no significant correlation between its duration with change in HRV parameters between the groups. There was no significant difference in HRV parameters between patients with long (>10s) and short (<10s) duration of IED. Conclusions : Transient increase in heart rate during IED phase was noted in patients with absence epilepsy. Longer duration of IED seems to be linked with significant tachycardia. While most HRV parameters did not reach statistical significance, standard deviation of RR intervals and triangular index was noted to be decreased during the IED phase and returns to pre-IED levels after the episode. Keywords: Absence seizures, autonomic nervous system, heart rate variability Introduction Activation of the autonomic nervous system is well known in patients with epilepsy during either electroconvulsive therapy (ECT) or spontaneous seizure. [1] Most studies have shown changes in cardiac autonomic parameters, to occur in more than 90% of patients with complex partial and generalized tonic-clonic seizures. Moreover the autonomic changes of the semiology and foci of seizure vary considerably. [2],[3],[4],[5] Autonomic dysfunction has also been noted in the interictal period and could be the only sign during this phase of clinical calm. [6],[7] Autonomic dysfunction is more prominent in patients with refractory epilepsy well as long-standing, well-controlled epilepsy and it might play an important role in the cause of sudden unexplained death in epilepsy (SUDEP). [6],[7] The heart rate variability (HRV) during a seizure can be calculated from ECG recorded simultaneously with electroencephalogram (EEG). HRV before, during and after the seizure can be an indicator of the sum of sympathetic and parasympathetic input to the heart. [8] Changes in HRV vary between seizure types and in temporal lobe seizures, increased sympathetic and decreased vagal heart rate modulation often precedes ictal EEG changes. [9] Rapid parasympathetic withdrawal might occur prior to seizure onset and a peak in sympathetic activation may occur at seizure onset. [10] Pre-ictal elevation of cardiac parasympathetic activity may be a marker for secondary generalization of seizures. [11] Seizure in absence epilepsy is brief, multiple and is considered a benign condition. The first study in 1959 by Krump and Gerardy noted that 64% of patients with absence epilepsy had clinical heart rate changes during ictus. [12] Subsequently, Longin et al. (2007) had studied the influence of generalized spike and wave discharges on HRV parameters in children. [13] In a study by O'Regan et al. (2005) on childhood epilepsies, heart rate abnormalities were detected in 26% of focal seizures and 48% of generalized seizures; however, they did not find any abnormalities in absence seizure. [14] There are no studies that have specifically attempted to look into HRV in patients with absence epilepsy during, before and after the interictal epileptiform discharges (IED) of 3-Hz spike and wave. In this paper, we attempt to characterize the HRV during pre-IED, IED and post IED states using qualitative, time domain and geometric methods in patients with absence epilepsy. Material and Methods This study was conducted at the National Institute of Mental Health and Neurosciences (NIMHANS), a university teaching hospital from South India. Retrospective EEG data from eight patients with a diagnosis of absence epilepsy, based on clinical and EEG features were analyzed. The seizure semiology and frequency were noted for each patient at the time of EEG from case notes. The EEG data was sampled at 256 Hz with 10-20 international system of electrode placement along with lead II, ECG and EMG leads. The EEG and ECG data was visually screened, truncated and processed using EEGLAB Toolbox for MATLAB (Ver 6.01b, Swartz Centre for Computational Neuroscience, Univ. of California, San Diego). The EEG records displaying the 3-Hz spike and wave seizure discharges from eight patients with absence epilepsy were identified and corresponding electrocardiogram (ECG) time series are obtained. The ECG was truncated into three epochs corresponding to the pre-IEDs, IED and post-IED periods. The pre-IED and post-IED lengths were taken of at same duration as that of IED. The randomly selected inter-IED epochs (ECG corresponding to seizure or IED free period of at least 2 min) of lengths similar to IED epochs were also obtained. One event for each patient was evaluated. The duration of seizure discharges was further classified as long duration (>10 s) and short duration (<10 s) based on IED epoch lengths. The raw ECG was converted into consecutive RR intervals for analysis. [Figure - 1] shows a sample of ECG and RR intervals corresponding to pre-IED, IED and post-IED in the EEG. Analysis was performed using HRV Analysis Software V1.1 (Biomedical Signal Analysis Group, Department of Applied Physics, and University of Kuopio, Finland). The following parameters were chosen as per the recommendations by the European Society of Cardiology, 1996. [8] 1. Time domain parameters:
2. The geometric parameter: Triangular index of RR interval (RR-TI) was also studied. To calculate the triangular index, the RR intervals are ordered into bins thus creating a histogram. The index is calculated by dividing the integral (area) of the distribution by its maximum height. Thus RR distributions with greater variability will have a more even spread and thus a smaller peak, the area to peak ratio will be larger than in case of a low variability and thus a clustered distribution. [8] Significant heart rate changes (bradycardia/tachycardia) were defined as a change more than 10 bpm from baseline. Statistical analysis All continuous variables were expressed as mean ± standard error of mean (SEM). The pre-IED, IED and post-IED groups were compared using repeat measure analysis of variance. Pearson's correlation was used to compare duration of seizure and HRV parameters. Independent sample't' test was used to compare HRV parameters between long- and short-duration seizure groups. Significance was set at P < 0.05 and trend at P < 0.1. Results There were three males and five females. Their mean age at evaluation was 13.0 ± 2.5 years (range: 6-26 years). The mean age at onset was 6.6 ± 1.2 years (range: 2-12 years) and the mean duration of illness at evaluation was 5.7 ± 2.7 years (range: 0.17-23 years). All patients had simple absence seizures. Six patients had daily seizures and other two had seizures at a frequency of greater than 1 per month. One patient was drug naοve, six were on sodium valproate, while one patient was referred to us with a combination of carbamazepine and clobazam. With medication at the time of EEG, seizures were controlled in two patients. All underwent routine scalp EEG recording and revealed the classical 3-Hz spike-wave discharges. Four patients had duration of IEDs less than 10 s, while the remaining four had duration of IED greater than 10 s. None of the patients had interictal tachycardia (HR > 100 bpm) and only one had pre-ictal tachycardia. Significant interictal to ictal tachycardia was noted in two patients. Both these patients belonged to the long-duration IED group. [Table - 1] shows the comparison of HRV parameters between different groups. The HR and triangular index varied significantly throughout the record while there was a trend in mean RR interval. There was a trend for tachycardia during the IED phase which returned to baseline during the post-IED phase. There was significant decrease in standard deviation of RR intervals and a trend in triangular index during the IED phase when compared to pre-IED phase. The percentage of RR intervals >50 ms was lower during the IED phase and achieved significance when compared to post-IED phase. The pNN50 and RRTI varied significantly between the post- IED and IED phases and there was a trend in mean HR and mean RR. There was no difference between HRV parameters between pre-IED and post-IED phases. The inter-IED mean HR (pre-IED: 90.15 ± 3.45 bpm, inter-IED: 86.93 ± 3.48 bpm, P = 0.038) was significantly lower while mean RR duration (pre-IED: 675.2 ± 25.95 ms, inter-IED: 700.4 ± 28.81 ms, P = 0.024) was higher than pre-IED values. Though not significant, inter-IED RRSD (pre-IED: 40.0 ± 4.15 ms, inter-IED: 34.6 ± 5.52 ms, P = 0.39) and RMSSD (pre-IED: 39.31 ± 5.68 ms, inter-IED: 37.28 ± 5.92 ms, P = 0.76) were lower than pre-IED values. We did not find any significant difference between inter-IED and pre-IED, pNN50 (pre-IED: 22.0 ± 6.24, inter-IED: 23.94 ± 7.41, P = 0.89) or RRTI (pre-IED: 0.05 ± 0.004, inter-IED: 0.06 ± 0.004, P = 0.29). While mean HR and mean RR interval during IED significantly correlated with the duration of ictus (r = 0.761, P = 0.028 and r = -0.750, P = 0.032 respectively), there was no significant correlation between the duration of IED with change in HRV parameters between pre-IED: IED and IED: IED phases. There was no significant difference in HRV parameters during IED between patients with short duration and long duration of IED, though there was a trend for tachycardia in subjects with long-duration IED. The mean HR, RRSD and RRTI in short duration IED was (86.56 ± 4.53 bpm, 25.5 ± 3.6 ms, 0.03 ± 0.004) and in long duration IED (103.08 ± 2.61 bpm, 35.3 ± 4.46 ms, 0.04 ± 0.002) with P values of 0.067, 0.276 and 0.351, respectively. Discussion HRV analysis is a valid method for quantifying central influences on autonomic cardiac changes, and can give valuable information when used as an adjunct during clinical seizures. However, the short duration of seizures and accompanying EMG artifacts are the primary reasons for the lack of application of these methods. The recommended epoch duration of the task force on HRV requires up to 1-2 min recordings to comment on the spectral components of HRV. Though a similar duration is recommended for time domain measures, short time records are also valid but may not give an accurate picture about the sympathetic-vagal balance. [8] Graphical representation of RR intervals [Figure - 1] in the eight patients with absence epilepsy clearly demonstrated a decrease in variability (seen as flattening of RR intervals) and increased HR corresponding to the IED. In five subjects [Figure - 1]b, c, e, g, h, this is visually identifiable and began either just before or shortly after onset of IED and might proceed for some period during the post-IED phase. There might be occasional rebound decrease in HR during the post-IED phase compared to pre-IED phase but the variability remained low. In the three subjects [Figure - 1]a, d, f where decreased HRV is not visually prominent, tachycardia and decreased variability occurs much earlier in the pre-IED and recovery to baseline is variable occurring by mid or late IED. The duration of seizure did not correlate with the degree of RR variability suppression. Larger number of samples with longer IED durations will be required to investigate this aspect. Parameters depicting sympathetic modulation such as the mean HR as well as those depicting parasympathetic modulation such as the RR-SD and RMS-SD were lower during the inter-IED period. These parameters increased during the pre-IED period and are suggestive of initial parasympathetic and sympathetic surge during the pre-IED phase in the EEG. This type of change has previously been documented in secondary generalized complex partial seizures. [11] There was significant decrease in standard deviation of RR intervals during IED phase when compared to pre-IED phase suggestive of parasympathetic withdrawal during ictus. Krump and Gerardy (1959) noted initial bradycardia followed by tachycardia in their patients with petit mal epilepsy which might have been due to loss of the pre-ictal parasympathetic surge and dominance of sympathetic activity. [12] The duration of IED did not affect the degree of HRV change between pre-IED: IED and IED: post-IED phases. The longer duration of epileptiform discharges in patients with absence of epilepsy are associated with more prominent behavioral arrests. As HRV changes are due to stimulation of central autonomic areas, longer duration of stimulation of autonomic areas follow a similar sympathetic, parasympathetic interplay as that of short duration seizures albeit on a longer timescale. The limitations are small number of patient's studied, short duration of analyzed segment and lack of analysis of effect of AEDs on HRV parameters. The role of AEDs and autonomic dysfunction in epilepsy remains controversial. Autonomic dysfunction in epilepsy was previously partly attributed to the use and withdrawal of anticonvulsants, especially carbamazepine which has been shown to decrease HRV and causes parasympathetic hypofunction. [15] Studies by Berilgen et al. have shown no significant association between autonomic dysfunction and the use of anticonvulsants. Berilgen et al. have also suggested that autonomic changes are amenable to antiepileptic medication. [16] The results of this study clearly demonstrate that autonomic dysfunction occurs during IEDs even in absence seizures. While the clinical phenomenon of SUDEP warrants the study of autonomic dysfunction in epilepsy patients, the very lack of consensus about the harm or benefits of AEDs poses clinical dilemma. Transient tachycardia was noted during the inter-ictal epileptiform discharges in patients of absence epilepsy characterized by reduced HRV. Longer duration of IED seems to be linked with significant tachycardia. While most HRV parameters did not reach statistical significance, standard deviation of RR intervals and triangular index was noted to be decreased during the IED phase and returns to pre-IED levels after the episode. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11006t1.jpg] [ni11006f1.jpg] |
| |||||||||

{kind=link}
{kind=link}