 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
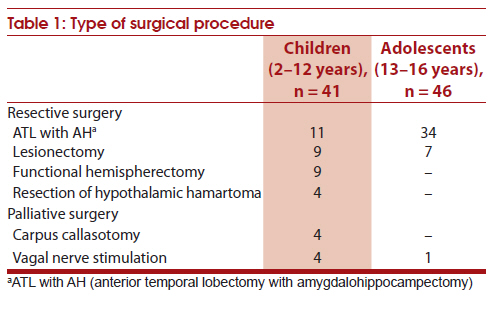
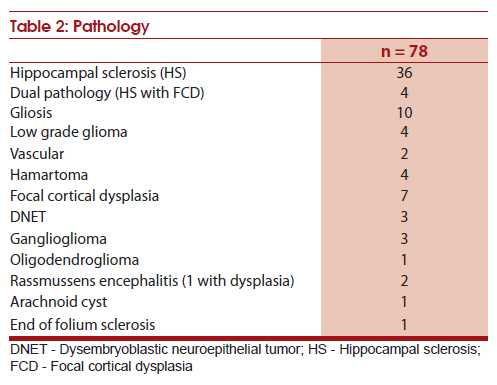
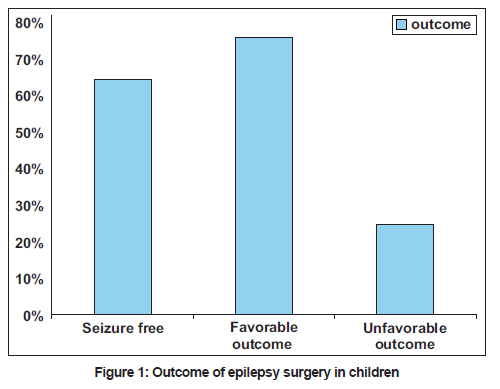
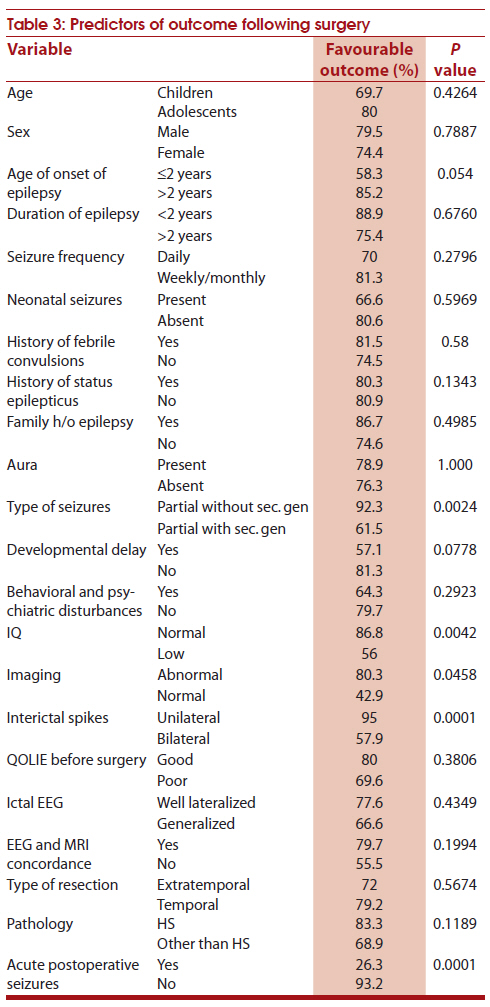
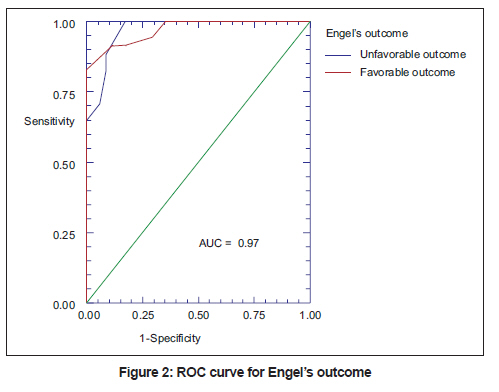
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 30-36 Original Article Outcome of epilepsy surgery in children after evaluation with non-invasive protocol Sita Jayalakshmi1, Manas Panigrahi2, Dilip Kumar Kulkarni3, Megha Uppin4, Shanmukhi Somayajula1, Sundaram Challa4 1 Department of Neurology, Krishna Institute of Medical Sciences, Hyderabad, Andhra Pradesh, India Date of Submission: 29-Jul-2010 Code Number: ni11007 PMID: 21339655 Abstract Objective : To assess outcome of epilepsy surgery in children with medically refractory partial epilepsy evaluated with non-invasive protocol and to determine the predictors of outcome.Patients and Methods : Retrospective analysis of presurgical, surgical, and postsurgical data was performed in 87 children who had at least 1 year post surgery follow-up. Outcome was assessed according to Engel's outcome classification. Stepwise regression followed by logistic regression analysis was employed in data analysis. Results : Mean follow-up was 32 (12-58) months and 44 (50.6%) were males. The age of onset of epilepsy was below the age of 2 years in 24 (30.8%). Resective surgery was done in 78 children. The commonest surgery performed was a temporal resection (88.9%) in adolescents and an extra-temporal resection ( 60.6%) in children. The commonest pathology was hippocampal sclerosis (HS) in adolescents and developmental, tumoral lesions, and gliosis in children. At last follow-up, 50 (64.1%) were seizure free and Engel's favourable outcome was noted in 59 (75.6%). After stepwise regression analysis, variables found to be significant (P < 0.05) and predicting a favourable outcome were lesion on MRI, normal IQ, and partial seizures without secondary generalization. Bilateral spikes on interictal EEG and acute postoperative seizures were predictors of poor outcome. A regression model was developed; the sensitivity, specificity, accuracy, and area under ROC curve were 82%, 91%, 88.5%, and 0.97%, respectively. Conclusion : Favourable outcome after epilepsy surgery can be obtained in children with temporal lobe epilepsy with HS and lesion-related epilepsies in developing countries with limited resources, after evaluation with a non-invasive protocol. Keywords: Epilepsy surgery, children, outcome, non-invasive Introduction Approximately 10-40% children with epilepsy will continue to have medically refractory epilepsy. [1],[2],[3] Surgery is an accepted choice of therapy in the management of refractory partial epilepsy in children. [4],[5],[6] Epilepsy surgery results in the control of seizures as well as psychosocial development. [4] Due to the advances in neuroimaging technologies, surgery can be considered in more than 50% of patients with refractory epilepsy. [7],[8] Most of the patients with substrate-directed intracranial lesions associated with chronic focal epilepsies can be selected for surgery based on relatively simple and affordable non-invasive evaluation strategy. [8] This will help in selecting more number of patients in resource poor countries. Completeness of resection is a significant predictor of good outcome in children. [9] Seizure-free outcome after epilepsy surgery in children is more frequent after temporal resection than after extra-temporal or multilobar resections and is comparable with results from adult series. [6],[10],[11] Normal intelligence and unifocal lesion on magnetic resonance imaging (MRI), tumor as etiology and older age at onset were associated with favourable outcome. [10],[12],[13] Multiple seizure types, preoperative developmental delay, bilateral or multifocal EEG findings, and those with temporal plus extra-temporal foci are predictors of unfavourable outcome after surgery. [14],[15] Outcome of epilepsy surgery depends on presurgical evaluation comprising a battery of invasive and non-invasive investigations. Invasive evaluation is frequently used in children, especially in those with extra-temporal resections and the results are less satisfactory. [16] In developing countries, extensive presurgical evaluation may not be possible due to limited resources. The objective of this study was to assess the outcome of epilepsy surgery in children with medically refractory partial epilepsy evaluated with non-invasive protocol and to determine the predictors of outcome following surgery. Patients and Methods Retrospective analysis of presurgical, surgical, and postsurgical data of 87 children (age: 2-16 years) who underwent epilepsy surgery between April 2003 and May 2009 and had at least 1 year post-surgery follow-up was performed. Resective surgery was done in 78 and 9 underwent palliative surgery. Presurgical evaluation Presurgical investigations and surgery were performed after patient's parents had given their informed consent. The presurgical evaluation included: detailed history of age of onset, type and frequency of seizures, neonatal seizures, febrile convulsions, and neurological examination. In children ages between 2 and 14 years, developmental quotient (DQ), social maturity, and intelligence quotient (IQ) were assessed using standardized tests namely developmental screening test, Vineland Social Maturity Scale, Binet-Kamath Intelligence Scale, and standard progressive matrices. Children from 15 to 16 years were assessed on intelligence and neuropsychological tests which included tests of attention, visuospatial, and memory functions. Montreal handedness test, behavioural problem assessment, and psychiatric evaluation according to ICD-10 were performed. Quality of life was assessed using QOLIE 48 in children aged 10-16 years and by parental interview based on children's behaviour, cognitive abilities, physical and neurological disability in the rest of the age group. Outcome variable QOLIE-48 was divided into two groups separated by median 50 (0-100 scale) into >50 as good outcome and <50 as poor outcome. Imaging of brain was done with 1.5 T MRI using appropriate sequences. All the children underwent prolonged video-EEG (VEEG) monitoring and at least two seizures were recorded. Ictal single photon emission computed tomography (SPECT) was performed in 34 children and 17 children underwent interictal fluoro deoxy-d-glucose positron emission tomography (FDG PET). Invasive monitoring was not used, and WADA test was not performed. Interictal spikes were grouped as unilateral (>75% on the ipsilateral side of the imaging abnormality) and multifocal. The ictal EEG patterns were classified as follows: focal-activity maximal at a single electrode with no more than two contiguous electrodes within 80-100% of the maximal activity; regional-activity involving electrodes overlying a single lobe having a 2:1 or greater amplitude predominance than that seen over other regions of the same hemisphere; hemispherical-lateralized activity involving multiple electrodes over multiple lobes of a single hemisphere having a 2:1 or greater amplitude predominance than that seen over the contralateral hemisphere; generalized-activity involving multiple electrodes over both cerebral hemispheres having a less than 2:1 amplitude predominance of one side over other. Surgery The type of surgeries performed were standard anterior temporal lobectomy with amygdalohippocampectomy (ATL with AH), lesionectomy, and functional hemispherectomy. Extra-temporal resections consisted of complete resection of the lesion combined with corticectomy. Intra-operative electrocorticography was used in 14 children. Acute postoperative seizures were defined as seizures occurring within 7 days of surgery. Outcome The outcome at the end of 1 year was assessed according to the Engel's classification. [17] Engel's class I and IIA outcome was grouped as favourable outcome. Data analysis Descriptive statistical analysis was performed. Initially, 22 variables were selected and stepwise regression analysis was done with NCSS 2007 Software to find out the variables which have independent influence on the outcome (P<0.05). Stepwise regression analysis is a combination of both forward and backward regression selection technique to decide which variables are having significant effect on outcome. After stepwise regression analysis, five variables were found to be significant (P<0.05) and a further analysis was performed by logistic regression analysis to develop an outcome model. The prediction model was assessed by sensitivity, specificity, and accuracy. Overall assessment was done by area under receiver operating characteristic (ROC) curve. Above 0.7 of area under the curve was considered to be diagnostically very useful. Results There were 87 children; 44 (50.6%) were males. The age at surgery was 2-16 (mean 12.07 ± 4.22) years. The duration of epilepsy was 1-16 (mean 7.24 ± 4.17) years. The mean age of seizure onset was 5.7 years (range, 1 day to 15 years). The age of onset of epilepsy was <2 years in 24 (27.6%). The average number of antiepileptic drugs (AED) received prior to surgery was 5.5 (range, 2-9). The seizure frequency was daily in 30 (34.5%). Twelve (13.8%) children had history of status epilepticus and 27 (31%) had febrile convulsions. Neonatal seizures were noted in 11 (12.6%). The mean follow-up was 32 (12-58) months. Presurgical evaluation MRI brain The MRI brain was abnormal in 80 (92%). There were seven children with temporal lobe epilepsy (TLE) and apparently normal MRI. The MRI was suggestive of mesial temporal sclerosis (MTS) in 32 (bilateral three), focal tumoral lesions in 13 and focal cortical dysplasia in 7. Hemispherical atrophy was noted in 6, Rasmussen's encephalitis in 3 and hemispherical dysplasia in 2. Four children had hypothalamic hamartoma (HH), and 1 had bilateral perisylvian polymicrogyria while 4 children had diffuse cerebral atrophy due to hypoxic-ischemic birth injury. Electrophysiological evaluation The interictal spikes were unilateral in 40 (46%) and bilateral or multifocal in the rest. The ictal EEG showed focal or regional onset in 44 (50.6%), hemispherical in 25 (28.7%), and generalized in 18 (20.7%). The ictal EEG onset was concordant with MRI in 69 (86.3%). Functional imaging Ictal SPECT was done in 34 children and interictal FDG PET in 17. All the children with normal MRI brain and those with discordance of MRI and electroclinical data underwent ictal SPECT and interictal FDG PET. IQ and quality of life The IQ was normal in 53 (60.9%); 21 (24%) had developmental delay. The quality of life was poor in 33 (37.9%) children prior to surgery. Behavioural and psychiatric problems were noted in 17 (19.5%). Psychiatric problems noted were attention deficit hyperactivity disorder (ADHD), dissociative disorder, and pseudo seizures. Behavioral problems noted were temper tantrums, stubbornness, and anger. Surgery Seventy-eight children underwent resective surgery. Temporal resections were more common 53 (67.9%) than extra-temporal resections; the commonest surgery performed was a temporal resection (40 of 45; 88.9%) in adolescents, and an extra-temporal resection (20 of 33; 60.6%) in children [Table - 1]. Functional hemispherectomy was performed in 9 (11.5%) children with hemispheric epilepsy. Palliative surgery was done in 9 children-corpus callosotomy in 4 and vagal nerve stimulation (VNS) in another 5. Repeat surgery was performed in one child with hemispherical dysplasia. Complications There was no mortality. Surgical complications were observed in 4 (5.1%) children. Transient hemiparesis was noted in one, one had transient third nerve palsy, and two had hemianopia. All the nine children who underwent hemispherectomy had worsening of their preoperative hemiparesis which improved and all are ambulatory. Asymptomatic quadrantanopia was noted in 50 (64.1%). Acute postoperative seizures occurred in 19 (24.4%) children. Histology The commonest pathology was hippocampal sclerosis (HS) noted in 36 (46%) followed by developmental abnormalities and tumoral lesions [Table - 2]. Outcome The outcome was analysed in the 78 children who underwent resective surgery. At the last follow-up, 50 (64.1%) were seizure free. The seizure freedom was better in temporal resections (38 of 53; 71.7%) than with extra-temporal resections (12 of 25; 48%). Engel's favourable outcome was noted in 59 (75.6%). Engel's favourable outcome was noted in 42 of 53 (79.3%) children after a temporal resection and 18 of 25 (72%) with extra-temporal resection; 7 of 9 (77.8%) children had favourable outcome after hemispherectomy and 2 of 4 (50%) with resection of hypopathalamic hamartoma. Children with HS on pathology (30 of 36, 83.3%) had the most favourable outcome. Favourable outcome was noted in 23 of 33 (69.7%) children and 36 of 45 (80%) adolescents, and the difference between the groups was not statistically significant [Figure - 1]. Hippocampal sclerosis was relatively more common in adolescents (22 of 45, 48.9%) while developmental, tumoral lesions, and gliosis were more common in children (21 of 33, 63.6%). Parents reported improved quality of life of children after surgery in 68 (87.2%). Four children with daily seizures underwent corpus callosotomy, two were seizure free, and two had remission of seizures by >90%. Five children had VNS implantation, 3 had remission by >50%, one by 40%, and no significant change in one. Three children with temporal lobe epilepsy had bitemporal ictal EEG onset (>30% seizures arising from opposite side), while four children had uncertain onset on ictal EEG. They were operated after a concordance of ictal SPECT and FDG PET with MRI brain. Five children were seizure free after surgery while another had favourable outcome. Three children had bilateral MTS on MRI. The interictal EEG showed bitemporal spikes. They were operated after a unilateral ictal EEG onset with a concordant ictal SPECT. The FDG PET showed unilateral hypometabolism in one and asymmetrical bitemporal hypometabolism in two, being marked on the side of ictal EEG onset. All the 3 children were seizure free at the last follow-up. Seven children had TLE and apparently normal MRI. Four had right temporal deficits, and 3 had left temporal deficits on neuropsychology. Surgery was done after a unilateral ictal EEG onset, unilateral interictal spikes on EEG with a concordant ictal SPECT and FDGPET with the ictal EEG onset. The histopathology showed HS in 6 and gliosis in 1. One child was seizure free, and another three had favourable outcome. Predictors of outcome Initially, 22 variables were recorded for developing regression model to predict the outcome of epilepsy surgery for Engel's favourable outcome. After stepwise regression analysis, five variables were found to be significant (P<0.05). The variables predicting a favourable outcome were abnormal imaging, normal IQ, partial seizures without secondary generalization, and unilateral spikes on interictal EEG. Occurrence of acute postoperative seizures was a predictor of poor outcome [Table - 3]. Then, logistic regression analysis was performed to develop a regression model to predict Engel's favourable outcome with these five selected variables. The regression equation is as follows: Engel's outcome = 18.950 - (36.396 Χ type of seizure) + (36.067 Χ IQ) + (1.813 Χ acute postoperative seizures) + (20.215 Χ Imaging) - (36.866 Χ interictal EEG spikes). The ROC curve for the model is shown in [Figure - 2]. The model assessment was evaluated by estimating the sensitivity (82%), specificity (91%), over all accuracy (88.5%), and the area under the ROC curve (AUC = 0.97). The sensitivity, specificity, accuracy, and AUC of the regression model developed are very high and diagnostically useful. Discussion This study indicates that favourable outcome after epilepsy surgery can be achieved in a good number of children with a simple non-invasive presurgical evaluation protocol. The seizure free outcome was noted in 64.1%, similar to the outcome of epilepsy surgery in children from previous series. [9],[10],[12],[13],[15],[16] Seizure free outcome was better in temporal resections (71.7%) compared to extra-temporal resections (48%). Engel's favourable outcome was achieved in 79.3% of temporal and 72% of the extra-temporal resections. This is similar to the outcome in previous studies. [6],[10],[11],[18],[19],[20] The presence of hippocampal sclerosis on pathology is associated with the favourable outcome (83.3%). Higher rates of seizure freedom can be obtained in children with TLE and HS, as demonstrated in the past. [11],[14],[21],[22] Histopathology of temporal resections in children usually reveals focal cortical dysplasia or tumoral lesions, and HS is less common. [10],[13],[22],[23] However, a few series on surgical outcome in children with focal lesions had HS as the commonest underlying pathology. [11],[24] In this study, the outcome was similar in children and adolescents, as reported previously. [10],[24] Adolescents had HS relatively more common and children had developmental, tumoral lesions, and gliosis as demonstrated in previous series. [10],[24] Nine children underwent hemispherectomy and 7 (77.8%) had favourable outcome. Although the number is small, the results are encouraging; 90% reduction in seizure frequency can be achieved in 89.5% of children after hemispheric surgery for refractory epilepsy. [25] The incidence of minor complications was 5.1%, and none had major complications and this is comparable to other pediatric epilepsy surgery series. [11],[13],[23],[26] Most of the children were operated relying on MRI brain and electroclinical information. Ictal SPECT and interictal FDG PET was performed in children with presumed temporal lobe epilepsy with normal MRI and those with a discordance of MRI and ictal EEG data. In pediatric patients with temporal lobe epilepsy, invasive monitoring using subdural or depth electrodes has been recommended when a consistent temporal seizure onset was not confirmed by ictal EEG or if the ictal EEG onset was unclear. [23] However, invasive EEG monitoring is expensive and is associated with complications such as intracerebral hemorrhage and infection. The outcome of temporal lobe surgery in this study was comparable to the outcome from previous series of temporal lobectomy in children without the use of invasive preoperative monitoring [27] as well as with the use of invasive monitoring. [13],[14],[26] Invasive monitoring is used more frequently in the evaluation of extra-temporal than temporal lobe epilepsies, [13],[16] and results are less satisfactory in spite of invasive monitoring. [16] MRI brain provides substantial information about the epileptogenic zone, especially when abnormal and a definite lesion is present, as seen in 92% of our cases. Non lesional cases will need extensive evaluation with functional imaging and invasive monitoring, especially in extra-temporal epilepsies. The statistical analysis showed that partial seizures without generalization and abnormal imaging are predictors of favourable outcome and the occurrence of bilateral interictal spikes, low IQ, and acute postoperative seizures are predictors of poor outcome. Not surprisingly, children with lesion on MRI had favourable outcome and normal imaging was a predictor of poor outcome as reported earlier. [10],[13],[14],[15],[19] Bilateral or multiple spikes on interictal EEG are associated with worse outcome, [14] suggesting a more diffuse process of epileptogenesis. However, most of these children had multiple seizure types and had significant remission following surgery and are probably unnecessarily grouped as surgical failures. Patients with normal IQ had better postoperative seizure outcome compared to those with low IQ, similar to previous reports. [12],[14],[28],[29] This probably suggests widespread disturbance of cerebral function in children with low IQ with unsatisfactory outcome following surgery. However, good outcome was obtained in children even with low IQ in some series. [3],[28] An acute postoperative seizure occurred in 24.4% in our series and was associated with poor outcome. In Cleveland Clinic series, acute postoperative seizures occurred in 26% and the risk was more in extra-temporal resections than hemispherectomy. It predicted a poor postoperative seizure outcome. [30] Acute postoperative seizures was found to be an independent predictor of less favourable outcome. [31] Four patients underwent corpus callosotomy and had >90% remission in seizure frequency. Five patients had VNS implantation, and three had >50% seizure remission. These numbers are too small to draw any conclusions. This study indicates that surgery is a valuable option to treat children with drug-resistant focal epilepsies, with 75.6% being free of disabling seizures. In developing countries with limited resources, favourable outcome can be achieved after presurgical evaluation with a non-invasive protocol in children with TLE with HS and lesion-related epilepsies. Lesion on MRI, normal IQ, and partial seizures without secondary generalization are predictors of favourable outcome. Bilateral spikes on interictal EEG and acute postoperative seizures were predictors of poor outcome. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11007f2.jpg] [ni11007t1.jpg] [ni11007t3.jpg] [ni11007f1.jpg] [ni11007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}