 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
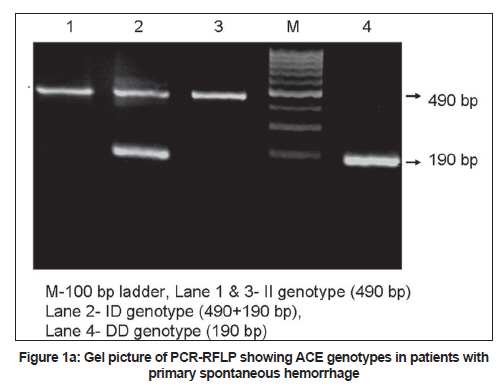
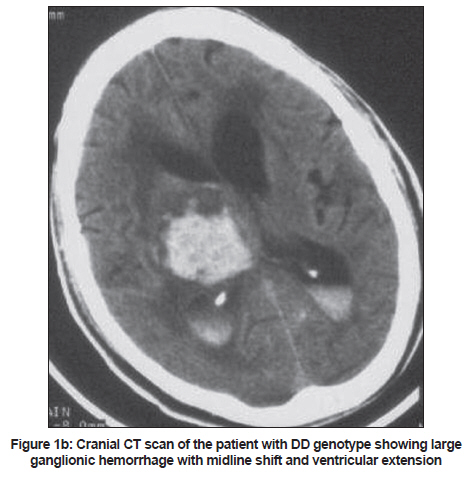
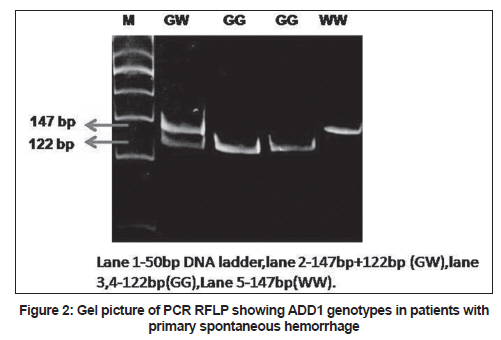
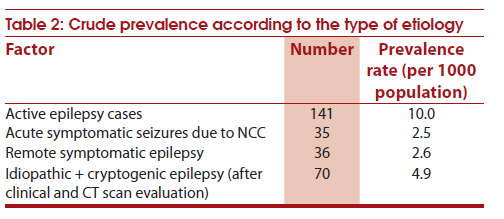
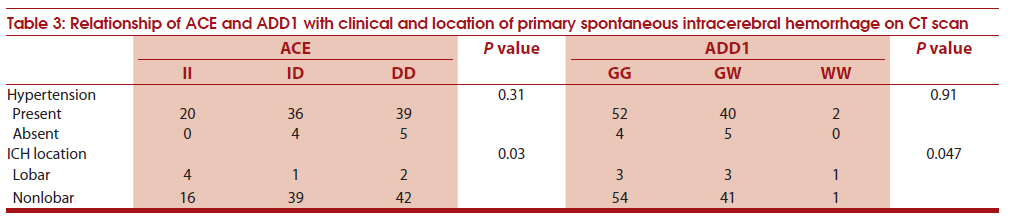
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 41-46 Original Article Angiotensin-converting enzyme (rs4646994) and α ADDUCIN (rs4961) gene polymorphisms' study in primary spontaneous intracerebral hemorrhage J Kalita1, UK Misra1, IS Bindu1, B Kumar1, B Mittal2 1 Department of Neurology, Sanjay Gandhi Post Graduate Medical Sciences, Lucknow, India Date of Submission: 06-Sep-2010 Code Number: ni11009 PMID: 21339657 Abstract Background : Primary spontaneous intracerebral hemorrhage (PSICH) is common in Asia and may have a genetic basis.Objective : To report the role of angiotensin-converting enzyme (ACE) and a ADDUCIN (ADD1) gene polymorphisms in patients with PSICH. Setting : Tertiary care teaching referral hospital. Patients and Methods : Study subjects included 104 patients with PSICH diagnosed by computed tomography (CT) brain scan and 198 controls. The vascular risk factors of stroke were noted. The location and size of the hematoma on CT scan were recorded. ACE (rs4646994) and a ADDUCIN (rs4961) gene polymorphisms were analyzed by polymerase chain reaction (PCR). The genotype and allele frequency were compared between patients and controls and within the PSICH group. Results : The median age of the PSICH group was 58 years, 17 (16.3%) patients were aged above 70 years and 40 (38%) were females. Ninety-three (91.2%) patients were hypertensive and 17 (16.5%) were diabetic. Hematoma was putaminal in 88 (84.5%), pontine in 5 (4.9%), cerebellar in 2 (1.9%), lobar in seven (6.8%) and multiple and primary intraventricular in one (1%) patient each. In the patients with PSICH, ACE DD genotype was present in 44 (42.8%) and ID in 40 (38.4%) whereas in controls these were 22 (11.1%) and 103 (52%) respectively. ADD1- WW genotype was found in two patients (1.9%), and GW in 44 patients (42.7%). In the controls these were found in nine (4.5%) and 65 (32.8%) respectively. DD genotype had 7.4 times higher risk of PSICH. ADD1 variant genotypes were not associated with increased risk but in association with ACE DD genotype resulted in significantly higher risk of PSICH. ACE and ADD1 variant genotypes were associated with nonlobar hematoma. Conclusion : ACE DD genotype in isolation or in combination with ADD1 GW genotype is associated with PSICH, especially nonlobar hematoma. Keywords: Angiotensin-converting enzyme, genetic study, hypertension, intracerebral hemorrhage, stroke, a ADDUCIN Introduction Intracerebral hemorrhage (ICH) may occur due to hypertension, vascular malformation, cerebral amyloid angiopathy (CAA), trauma and coagulopathy. The commonest cause of primary spontaneous intracerebral hemorrhage (PSICH) in the young is hypertension and in the elderly CAA. Hypertension is an important cause of ganglionic, pontine and cerebellar hemorrhages [1] and can as well be the cause of lobar hemorrhage. [2] The arterial pathophysiology of hypertensive ICH is lipohyalinosis of small deep penetrating cerebral blood vessels and rupture of micro aneurysms. [3],[4],[5] Lipohyalinosis has also been reported in the brain of normotensive patients with recurrent ICH. [6] A minority of patients with deep PSICH may be normotensive. [7] Similarly, lobar hemorrhage in the elderly though attributed to CAA may as well be caused by hypertension. A number of candidate genes have been associated with hypertension and vasculopathy. Angiotensin-converting enzyme (ACE) is the rate-limiting enzyme of the rennin angiotensin system and is involved in vascular remodeling and atherosclerosis. A single copy gene encoding ACE lies on Chromosome 17q and has two polymorphic alleles depending on insertion (I) and deletion (D) of 289 bp alu sequence in intron 16. PSICH has been associated with D allele of ACE gene. [8] a ADDUCIN (ADDI), a heterodimeric actin-binding protein exerts a complex biological effect on sodium and involve in homeostasis by interacting with sodium channel, sodium potassium chloride co transporter and sodium, potassium ATP system. [9] A single nucleotide ADDI polymorphism coding the substitution of tryptophan in place of glycine is associated with elevated blood pressure and salt sensitivity. [9],[10] In a Chinese study, W allele of ADD1 has been significantly associated with ICH and was independent of hypertension. [11] In the available medical literature there is paucity of genetic studies in ICH. ACE and ADD1 gene are known to be associated with hypertension, moreover hypertension is an important risk factor of ICH. The present study evaluates the association of ACE and ADD1 gene polymorphism in patients with PSICH and correlates these with clinical severity and radiological parameters. Patients and Methods Consecutive patients with computed tomography (CT)-proven PSICH admitted to the neurology ward at the Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India, during 2007 to 2008 were enrolled in the study. The patients with head injury, coagulopathy, vascular malformation, aneurysm and tumor bleed were excluded. A detailed medical history was obtained regarding the history of hypertension, diabetes mellitus, smoking, alcohol consumption, tobacco and family history of stroke in first-degree relatives. Admission blood pressure was recorded and evidence of retinopathy, cardiac hypertrophy and renal failure was also noted. Patients' consciousness was assessed by Glasgow Coma Scale (GCS) score. The control group included 129 males and 69 females without neurological deficit and history of hypertension, diabetes and coronary artery disease who belonged to the same geographic and ethnic groups of northern India. The mean age of the males in the control group was 54.3±9.7 years and in females 55.7±12 years. This study was approved by the Institute Ethics Committee (PG1/EP/EC/2007). Informed consent was taken from the controls and the patients or from their first-degree relative. Investigations Complete blood picture, blood biochemistry, prothrombin and activated partial thromboplastin time, radiograph of chest and electrocardiogram were done. Cranial CT scan was performed on a third-generation CT scanner and 10-mm sections were obtained parallel to the orbitomeatal line. On CT scan, the location of hematoma, volume, midline shift and ventricular extension of ICH were noted. The size of the hematoma was calculated as a x b x c/2, where a= largest diameter of hematoma in cm, b= diameter in cm perpendicular to a, and c=number of parenchyma hemorrhages seen in 1-cm slices. [12] The hematoma was classified into small < 20 ml, medium 20-40 ml and large >40 ml. Patients with normal blood pressure, lobar ICH and all the patients below 40 years were subjected to magnetic resonance (MR) angiography or digital subtraction angiography to exclude vascular malformations. Death during hospital stay and its probable causes were noted. Genetic study ACE (rs4646994) and ADD1 (rs4961) gene polymorphisms analysis Five ml blood from the antecubital vein was collected in ethylene diamine tetra acetate (EDTA ) vial and DNA was isolated from leukocytes by Miller's salting out method. [13] The I/D polymorphism analysis in the intron 16 of the ACE gene (17q23) was done by using 200 ng of DNA by polymerase chain reaction (PCR) using primers forward 5′CTGGAGACCACTCCCATCATTTCT3′(F) and reverse primer 5′GATGTGGCCATCACATTGGTCAGA 3′(R). An insertion-specific primer 5′TGG GAC CAC AGC GCC CGC CAC TAC3′ was also used to avoid DD misgenotyping. [14] Genotyping of ADD1 Gly460Try was determined by using primers forward 5′CTCCTTTGCTAGTGACGGTGATTC3′ (F) and reverse 5′GACTTGGGACTGCTTCCATTCGGCC 3′(R) using 200 ng of DNA in a reaction mixture of 25μl containing 20 pmol primers and 1U of Taq DNA polymerase enzyme using 200mM dNTPs. PCR cycle condition consisted of an initial denaturation step at 94ºC for 5 min followed by 34 cycles of denaturation at 95ΊC for 30 sec and 62ºC for 30 sec annealing for ACE PCR and 63ºC for ADD1 which was followed by extension at 72ºC for 25 sec and final elongation at 72ºC for 5 min (MJ Research PTC 200 Peltier Thermal Cycler). After amplification, PCR products were checked on agarose gel. Insertion /deletion polymorphism of ACE gene was checked by loading 5μl PCR product on 3% agaore gel. A PCR product of 490 bp showed a presence of the Alu insertion (I allele) while 190 bp fragment represented absence of insertion (D allele). Restriction digestion for ADD1 polymorphism was carried out in 25 ml volume with restriction enzyme Sau 961. Genotyping was carried out on 15% polyacrylamide gel. Restriction digestion products were run on polyacrylamide gel for 7 h at constant 200 V. On ethidium bromide staining and exposure to UV transilluminator, genotypes are represented by the following band pattern- W/W 460, 147 bp, G/W (147, 122 and 25bp); and G/G 460 122 +25 bp. [15] Statistical analysis The genotype and allele frequency of ACE and ADD1 in patients and controls was determined by direct counting. Hardy Weinberg equilibrium in controls was checked by Chi square test. The difference in the frequency of ACE and ADD1 genotype and allele was evaluated in patients and controls using binary logistic regression analysis and Mann Whitney U test. The genetic abnormalities in patients with and without hypertension and lobar and nonlobar ICH were also analyzed. The combination of various genotypes and alleles of ACE and ADD1 were also analyzed in patients and controls by Chi square test and the effect was evaluated with reference to location, size of hematoma and mortality. The variables were considered statistically significant if two-sided P value was < 0.05. Statistical analysis was done using SPSS 12 version and EpiInfo software. Results In patients with ICH, ACE genotyping was done in 104 and ADD1 in 103 as in one patient DNA sample had technical error during ADD1 analysis. ACE and ADDI genotyping was done in 198 controls. The median age of the patients was 58 (27-91) years; 16.3% were above 70 years of age and 40 (38.5%) were females. History of hypertension was present in 58 (55.9%) patients but after the ictus and during follow-up 93 (91.2%) patients were detected to be hypertensive. Admission systolic blood pressure ranged between 100 mmHg and 260 mmHg, and diastolic blood pressure between 60 mmHg and 170 mmHg. Seventeen (16.5%) patients were diabetic, 22 (21.4%) took alcohol, 24 (23.3%) chewed tobacco and 16 (15.5%) smoked. Past history of stroke was present in 22 (21.3%) patients. Admission GCS score ranged between 3 and 15 (median 9). Majority of the patients had severe stroke. The median Canadian Neurological Stroke Scale score was 2.5 (range 0.5-15). On CT scan, hematoma was in the basal ganglia in 88 (85.4%), pons in 5 (4.9%), cerebellar in 2 (1.9%), lobar in 7 (6.8%), and multiple and primary intraventricular in 1 (1%) patient each. Hematoma volume ranged between 4 and 118 (median 38) ml. Hematoma was large in 23 (22.5%), medium in 42 (41.2%) and small in 47 (36.3%) patients. Twenty-seven (26%) patients died in the hospital. Genetic analysis Analysis of ACE genotype revealed II genotype in 20 (19.2%), ID genotype in 40 (38.4%) and DD genotype in 44 (42.3%); whereas in the controls, these were 73 (36.9%), 103 (52%) and 22 (11.1%) respectively [Figure - 1]a. Presence of DD genotype resulted in 7.4 times higher risk of PSICH compared to wild genotype (OR 7.04, 95% CI 3.44-14.44, P = 0.001) [Figure - 1]b. D allele was present in 38.5% of patients and I allele in 61.5%. Presence of D allele was significantly associated with ICH compared to I allele (OR 2.69, 95% CI 1.92-3.84, P = 0.001). Analysis of ADD1 genotype revealed GG genotype in 57 (55.3%), GW in 44 (42.7%) and WW in 2 (1.9%) patients and in the control group these were 124 (62.6%), 65 (32.8%) and 9 (4.5%) respectively [Figure - 2]. The presence of a variant allele of ADD1 did not increase the risk of ICH. Similarly, G and W alleles were also not significantly different in patients and controls. The details are summarized in [Table - 1]. Gene-gene interaction revealed significantly higher association of DD and GW genotypes (OR 6.77, 95% CI 2.73-16.79, P = 0.0001). Combination of WW and ID genotypes however was not significantly related to ICH (OR 0.47, 95% CI 0.05-4.14, P = 0.50). The various genotype combinations of ACE and ADD1 are shown in [Table - 2]. ACE variant genotype was not related to hypertension (P=0.31) but was significantly associated with nonlobar hematoma (P=0.03). Similarly, ADD1 genotype was not related to hypertension but variant alleles were associated with nonlobar hematoma (P = 0.047). The details are summarized in [Table - 3]. ACE was not significantly related to CNS score ( P = 0.15), ICH volume (P = 0.12) and GCS score (P = 0.08). ADD1 was also not significantly related to the CNS score (P = 0.04), and ICH volume (P = 0.44) but was related to GCS score (P = 0.02). Discussion In the present study, DD genotype of ACE and its association with GW genotype of ADD1 increased the risk of PSICH. In a study in the Polish population, the evidence of ACE DD genotype was an independent risk factor for PSICH and not for small-vessel disease. [8] ACE plays an important role in the endothelial functions, replication of smooth muscle proliferation and tone as well as it may be involved in atherosclerosis. [16] The DD genotype has been associated with myocardial infarction [17] and stroke. [18] However, there are many reports with conflicting results about the role of ACE DD genotype as a risk factor for spontaneous ICH. A study reported negative association of ACE polymorphism with spontaneous ICH. [19] We have diagnosed ICH on CT scan and MR angiography was done in the patients who were young (<40 years), normotensive or had lobar ICH. Therefore, the other causes of ICH such as arteriovenous malformation, aneurysm and tumor bleed are unlikely. Moreover, 93.2% of our patients had deep-seated ICH, usually due to hypertension and only seven patients had lobar ICH. The etiology of lobar and deep-seated PSICH may be different. The deep brain ICH is mainly due to hypertension and more common in Asian countries whereas the lobar ICH in the elderly is due to cerebral amyloid angiopathy and may have a different pathophysiological basis. The DD genotype seems to influence PSICH independent of hypertension. A similar observation was made in another study. [20] Plasma ACE concentration has been associated with DD genotype but not with ID genotype and in the study of Slovik et al.[8] , it contributed to PSICH independent of hypertension. In our study also, ACE polymorphism was associated with PSICH and not with hypertension; however, only nine out of 103 patients were nonhypertensive. A larger sample may be needed to look for the association of ACE and ADD1 with hypertension, as hypertension is more prevalent in the population than ICH. ADD1 polymorphism was not associated with PSICH or hypertension but a combination of GW genotype of ADD1 with DD genotype of ACE was associated with PSICH in our study. In a Chinese study, W allele of ADD1 was associated with ICH independent of hypertension but we did not find such an association. It was interesting to note that the combination of both ACE and ADD1 homozygous genotype was not found in our patients. The present study underscores the association of the DD genotype of ACE and GW genotype of ADD1 in Indian PSICH patients. However, in an another study, the prevalence of W allele among ICH patients was 82% which was significantly higher than the controls and was independently associated with ICH. [11] In a longitudinal study on the occurrence of hypertension in a Belgian population, carriers of ACE DD genotype had a slightly higher incidence of hypertension compared to ID and II genotype. This small difference was increased to 250% when ADD1 and CY 11B2 polymorphisms were taken into account. [21] In our study, the ACE DD genotype in isolation or in combination with ADD1 GW genotype was associated with PSICH, especially in nonlobar hematoma. It is possible that ACE and ADD1 may interact leading tof enhanced susceptibility to PSICH. Our sample size is small for subgroup analysis, therefore these results need to be verified in a larger study. Acknowledgment We thank Indian Council of Medical Research, New Delhi for funding assistance. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11009t3.jpg] [ni11009f1a.jpg] [ni11009t2.jpg] [ni11009t1.jpg] [ni11009f2.jpg] [ni11009f1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}