 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
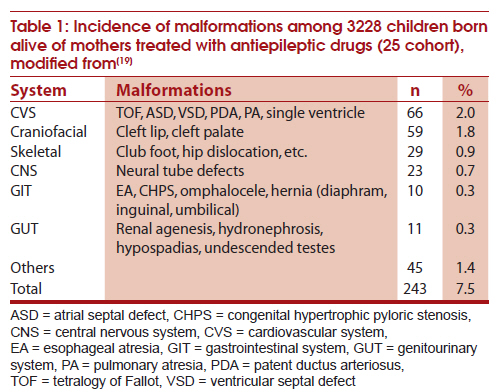
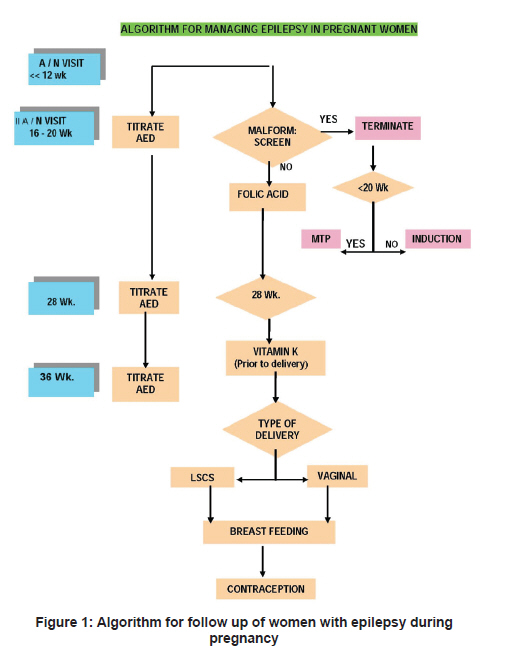
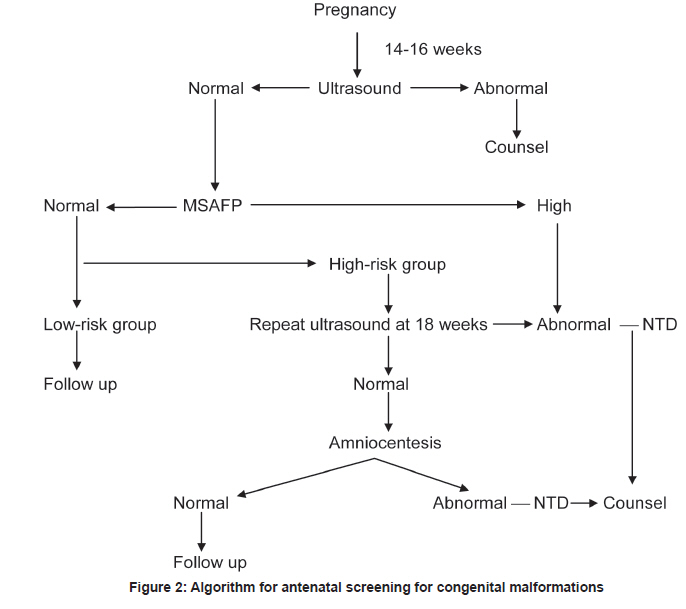
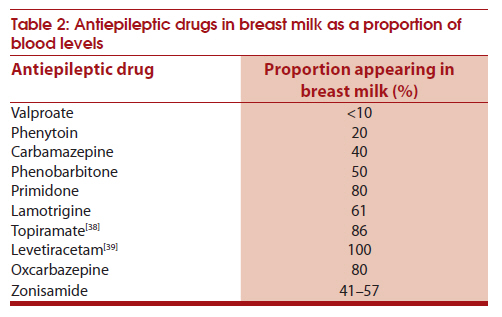
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 59-65 Topic of the Issue: Review Article Managing epilepsy in pregnancy Sanjeev V Thomas Kerala Registry of Epilepsy and Pregnancy, Department of Neurology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, India Date of Submission: 24-Jan-2011 Code Number: ni11013 PMID: 21339661 Abstract There are close to one and half million women with epilepsy (WWE) in reproductive age group in India. WWE have several unique gender-specific problems in the biological and social domains. Women experience more social stigma from epilepsy and have more difficulty with education and employment. They have more difficulty to get married and sustain successful family life. Reproductive hormones like estrogen and progesterone have opposing effect on seizure threshold. WWE have increased risk of infertility. About 10% of their babies may have major congenital malformations. Most of the adverse biological outcomes for WWE are related to adverse effects of antiepileptic drugs (AEDs). Traditional AEDs like phenobarbitone and sodium valproate are probably associated with increased risk of fetal malformations or other adverse fetal outcomes. Polytherapy and use of high dose of any AED is associated with higher risk fetal complications. It is very important that all WWE have a preconception evaluation done by a neurologist, when the need to continue AEDs or possibility of reducing AED load could be assessed. All WWE need to take folic acid 5 mg daily during preconception period and pregnancy. They should undergo a detailed screening for fetal malformations between 12 and 18 weeks of pregnancy. The neurologist, gynecologist, imageologist and pediatrician need to work as a team while managing pregnancy in WWE. It is important to reassure WWE and their relatives that pregnancy is safe in WWE and their children are healthy in more than 90% instances.Keywords: Antiepileptic drugs, pregnancy, teratogenic effects, women with epilepsy Introduction Epilepsy is the most common neurological disorder. There are about 50 million people with epilepsy worldwide and half of them are women. About a sixth of women with epilepsy (WWE) in the world are living in India. In India, it is estimated that there are about 2.73 million WWE and 52% of them are in the reproductive (15-49 years) age group. WWE experience more psychosocial problems and burden related to epilepsy than men. The social stigma associated with epilepsy is more severe for women than for men with epilepsy. Women have increased risk of marital issues, separation from spouse, divorce and social stigma, when compared to men with epilepsy. [1] Reproductive issues are one of the major concerns for WWE and their relatives. In this article, some aspects of epilepsy and reproductive issues as applicable to WWE are discussed. There are several ways by which epilepsy and its treatment influence reproductive functions and vice versa. Strategically located epileptogenic lesions can disturb the hypothalamo-pituitary axis. Antiepileptic drugs (AEDs) may interfere with the metabolism of sex hormones. Reproductive hormones have important influence on epileptogenesis. In experimental models, estrogen lowers the electroshock seizure threshold and creates new epileptogenic foci when it is applied topically over the cerebral cortex. In women with partial seizures, intravenously administered estrogen enhances the epileptiform activity in the EEG. Progesterone has the opposite effect of estrogen on neuronal excitability and epileptogenesis. The anticonvulsant property of progesterone is largely exerted through its metabolite, allopregnanalone, which is a gamma-amino butyric acid (GABA) A receptor modulationg neurosteroid. Progesterone may have a more direct antiseizure effect mediated through the progesterone receptors that account for most of its biological effects. Progesterone knockout mice failed to demonstrate the protective effects of progesterone when submitted to seizure challenge by pentylenetetrazol (PTZ) or maximal electroshock. [2] Catamanial Epilepsy About 30% women report predilection for seizures to occur at certain phases of menstrual cycle, which is referred to as catamenial epilepsy. In a recent study carried out in 100 women, it was observed that women had higher chance of seizures during ovulatory cycles (77%) than anovulatory cycles (20%). [3] There are other differences in the seizure pattern between ovulatory and anovulatory cycles. In that study, ovulatory seizures tended to occur at the onset of menstrual period (circaluteal rhythm) while anovulatory seizures tended to occur at the onset of menstrual period as well as around day 14 and day 9 of menstrual cycle. Infertility It was suspected that WWE may have reduced fertility, but the same was attributed to the lower marriage rate in them. A recent prospective study in epilepsy and pregnancy registry over 10 years had shown that WWE have increased risk of infertility, particularly if they are using polytherapy. Infertility was least (7.1%) for those with no AED exposure and higher (P = 0.001) for those with AED exposure (31.8% with one AED, 40.7% with two AED, and 60.3% with three or more AED exposure). In this study, WWE exposed to phenobarbital had significant risk of infertility, but no such trend was observed with valproate or other drugs. [4] AEDs can alter the reproductive hormone balance in women by several mechanisms. Valproate is known to alter the sex hormone metabolism and predispose to polycystic ovarian syndrome which in turn could lead to infertility. Enzyme inducing AEDs may increase the metabolism of estrogen and progesterone. AEDs may displace these hormones from the sex hormone binding globulin. Sexual disturbances and reproductive dysfunctions can often occur in WWE. These issues need to be explored in all women of reproductive age group. In certain situations, where endocrine dysfunction is clearly demonstrated, a change of AED may be required. [5] Effect of Pregnancy on Epilepsy Pregnancy can have variable effects on seizure frequency. Seizures may decrease or remain unchanged in two-thirds of patients. [6] In the European pregnancy registry of more than 1900 pregnancies in WWE, close to 60% had remained seizure free during pregnancy. [7] Women who had focal epilepsy or were using polytherapy had higher risk of seizures during pregnancy. In that series, 17.3% had aggravation of seizures while 15.9% experienced seizure reduction. Risk of seizures is the highest during delivery. [8] Status epilepticus can happen in less than 1% of patients. Effect of Epilepsy on Pregnancy A variety of complications of pregnancy have been reported in WWE. The data from Kerala Registry of Epilepsy and Pregnancy indicate that anemia, ovarian cyst and fibroid uterus, and spontaneous abortions are more frequent in WWE. [9] Population based data from Norway indicate that WWE have increased risk of induction of labor, cesarean section and postpartum hemorrhage. This risk was higher when the women were using AEDs than when not taking AEDs. [10] For WWE without AED use, the risk of cesarean delivery is slightly increased but risk for any other complications is not considerably increased. Effect of Epilepsy and AED on Fetus The adverse effects of epilepsy and AEDs on the fetus can be broadly classified as (1) anthropometric changes, (2) physiological changes, (3) teratogenic effects, and (4) long-term cognitive effects. Several studies have shown that infants of WWE have low birth weight and are small for gestational age. A large population-based study in Norway had shown that infants of WWE exposed to AEDs in utero had higher risk of preterm birth, low birth weight, intrauterine growth retardation, and smaller head circumference at birth. [11] Similar findings in birth weight were observed in neighboring Sweden also. [12] Head circumference at birth in infants of WWE is influenced by the paternal head circumference, maternal AED exposure and several other factors. [13],[14] Apgar score at birth is a reliable measure of the physiological status of the newborn. Population-based studies in Norway had revealed that infants exposed to AEDs in utero of mothers with epilepsy had lower Apgar score. [10] Teratogenic Effects Mechanisms of teratogenesis The most important concern regarding the use of AEDs during pregnancy is the potential risk of major congenital malformations in the offspring. There are several possible mechanisms for occurrence of congenital malformations in the fetus. These include genetic predisposition to malformations in the infants of WWE, direct effects of seizures, indirect effect of seizures such as falls and injuries, poor antenatal care, and teratogenic effects of AEDs. Data from the Kerala Registry of Epilepsy and Pregnancy had shown that there is no familial tendency for congenital malformations in the first and second degree relatives of WWE when compared to their spouses who do not have epilepsy. [15] Seizures can lead to reduced placental circulation and secondary ischemia in the fetus. Optimal reperfusion after the circulation is restored can lead t o increased oxidative stress, which in turn could exert teratogenic effects. Nevertheless, the most important modifiable factor related to teratogenesis in WWE could be the exposure to AEDs. The first case of malformation related to AED exposure was cited by Janz in German literature. Subsequently, several malformations have been described in association with exposure to phenobarbitone, phenytoin, carbamazepine and sodium valproate. There are several mechanisms by which AEDs may exert teratogenic effects. AED usage may lead to folate deficiency which in turn may predispose to neural tube defects. [16] There are other mechanisms such as increased oxidative stress related to the metabolism of AEDs. [17] AEDs that are metabolized by cytochrome P450 family of enzymes in the liver increase the levels of arene oxides as a byproduct of its metabolism. Arene oxide is a potent teratogen. Other mechanisms under consideration include alteration in the homeobox (HOX) genes, retinoic acid signaling pathways, histone deacetylators and polymorphisms involving AED transporters. [18] AED induced malformations can affect almost all organs [19] [Table - 1]. AED usage during pregnancy increases the risk of fetal malformations. [20] Data from pregnancy registries in USA and the Netherlands indicate that exposure to AEDs in the first trimester increases the risk of major congenital malformations. The odds ratio for malformations was 2.6 [95% confidence interval (CI) 0.8-8.3] with monotherapy exposure and 5.1 (95% CI 1.0-21.1) with polytherapy. [21] A meta-analysis of 65,000 pregnancies drawn from 59 studies revealed that malformation rate is increased for WWE. [22] Nevertheless, population-based studies of unselected WWE in Norway and Taiwan failed to demonstrate any excess incidence of major congenital malformations in their offsprings. [23],[24] The second issue is whether polytherapy carries increased risk when compared to monotherapy. Data from UK pregnancy registry had shown that risk of malformation is 3.7% (95% CI 3.0-4.5) while that associated with polytherapy is 6.0 (95% CI 4.5-8.0). [25] Increased risk associated with polytherapy had been observed with other registries and meta-analysis also. There is some controversy regarding the risk associated with specific AEDs. The population-based data from Norway showed that excess risk of malformations was associated with only valproate exposure. [18] In the UK pregnancy registry, malformation risk was higher for valproate (6.2%; 95% CI 4.6-8.8) when compared to phenytoin (3.7%; 95% CI 1.3-10.2), lamotrigine (3.2%; 95% CI 2.1-4.9) or carbamazepine (2.2%; 95% CI 1.4-3.4). [20] The Eurocat analysis had shown that valproate exposure is associated with increased risk of malformations, particularly for neural tube defects, atrial septal defect, cleft palate, hypospadias, polydactyly and craniosynostosis. [26] The case control comparisons in this study had revealed that the malformation risk associated with valproate monotherapy was significantly higher than that associated with exposure to other AEDs as monotherapy and exposure to no AEDs. The risk of major congenital malformations is higher when the fetus is exposed to any AEDs when compared to no exposure. There is fairly good agreement that polytherapy carries higher risk than monotherapy. Within monotherapy, the risk scales up as the exposure dosage increases, particularly for valproate and lamotrigine. Epidemiological studies (unselected population) have shown that folate deficiency increases the risk of neural tube defects and folate supplementation reduces this risk. The overall social mileu and access to health and social support mechanisms have also important bearing on congenital malformations. Long-term cognitive outcome Until recently, little attention had been paid to the long-term adverse effects of prenatal AED exposure on neurocogntive development of infants. Prospective data from the Kerala Registry of Epilepsy and Pregnancy had shown that a third of infants of WWE had impaired mental and motor development when assessed at 15 months of age. [27] Further, when these children were examined at 6 years of age, when more detailed neuropsychological and language testing were possible, they demonstrated significantly lower IQ and language performance when compared to age-matched control children without prenatal AED exposure or maternal epilepsy. [28] Similar were the observations in other registries also. [29] Older children of mothers with epilepsy in the UK required additional educational assistance significantly more often than others. [30] Exposure to polytherapy and valproate in high doses were associated with increased risk of neurocogntive developmental problems. Management of epilepsy and pregnancy The management of epilepsy and pregnancy needs to commence when the woman begins her reproductive life. It is ideal that the woman consults her neurologist while preparing for her marriage. There is often much pressure to discontinue AED usage prior to marriage because of the stigma and fear of adverse effects on pregnancy. Every woman with epilepsy needs to be carefully reassessed at this point of time. The neurologist should take this opportunity to reconfirm the diagnosis. It is not unusual to find that some women were inadvertently labeled as epilepsy, when they might have had syncope or other nonepileptic disorders. A good number of women are in remission and are candidates for AED withdrawal. The general principles of AED withdrawal in persons who are in remission can be followed in such situations. These women who do not have epilepsy can safely be weaned off AEDs. The risk of recurrence of seizures, particularly during the stress of marriage, and its impact need to be carefully appraised while considering AED withdrawal. Persons with juvenile myoclocic epilepsy (JME) may need to continue a small dose of AED as they carry high risk of relapse of seizures if the AEDs are completely withdrawn. Women who can potentially become pregnant need to be started on folic acid 5 mg daily, 1 or 2 months prior to anticipated pregnancy. Women often require counseling on several important issues: (1) the need to continue AEDs in order to remain seizure free; (2) reassurance that more than 90% of infants born to mothers with epilepsy and taking AEDs are healthy; (3) the risk of major congenital malformations is only to the tune of 6-8% and they occur mostly when the women are taking high dosage of medicines and multiple AEDs; this risk can be reduced by reducing the dosage or number of drugs and by using folic acid regularly during pregnancy; (4) all WWE should report to the physician and gynecologist as soon as they become pregnant and follow the instruction during pregnancy; and (5) it is probably not safe to abruptly discontinue medicines as soon as they become pregnant. Based on the observations in animal models, the teratogenic effects and developmental consequences observed in prospective registry based studies in WWE, FDA has reclassified valproate under Class D risk during pregnancy, which states that studies in pregnant women have demonstrated a risk to the fetus and its use in women in child bearing potential requires that the benefits of its use be weighed against the risk of injury to the fetus. Based on the observations and these recommendations, it may be preferable to avoid the use of valproate in women of childbearing potential, if an alternative is available and acceptable. Management of pregnancy and epilepsy Professional bodies have come out with guidelines and practice parameters to manage pregnancy in WWE. [31],[32],[33],[34] The Indian Epilepsy Society has published its guidelines for the management of epilepsy and pregnancy. [35] The general outline to manage epilepsy and pregnancy is given in the flow chart [Figure - 1]. WWE need to continue AEDs during pregnancy under supervision. In the first trimester, it is preferable to keep the dosage as low as possible in order to reduce the risk of malformations. Some women, particularly those taking oxcarbazepine or lamotrigine, may require dose escalation in the second half of pregnancy, as the blood levels of these AEDs tend to drop significantly with hemodilution and other metabolic changes. Our policy is to increase the dose only if there is break through seizures. Some women may require higher dose of AEDs near term and while in the labor room. If required, injection lorazepam can be used to abort seizures during pregnancy, particularly during labor. In the postpartum period, lamotrigine dosage may have to be reset to that of the early pregnancy, if the dosage had been increased during pregnancy. This is necessary because the blood level of lamotrigine tends to increase rapidly in this phase. Screening for fetal malformations Screening for major congenital malformations is an important aspect of antenatal care for WWE. Most of the organogenesis occurs before 10 weeks of pregnancy. An ideal screening test would be simple, safe and rapid to administer and economical. It should have high specificity and sensitivity. There are three possible procedures: (1) serum markers, (2) ultrasonography, and (4) amniotic fluid analysis. Current techniques of ultrasonography allow us to detect malformations reliably only by 12 weeks. Obstetricians carry out ultrasonography in early pregnancy before 8 weeks of pregnancy, mainly to document pregnancy and to confirm intrauterine location of product of conception. Usage of transvaginal probe increases the yield of early ultrasonography. A detailed ultrasonography, preferably carried out by an experienced imageologist, is necessary to document fetal anatomy carefully. By about 18 days after fertilization, the neural plate is formed. This subsequently folds in to the neural fold and starts to fuse in the central area. The rostral neuropore closes by day 24 and the caudal neuropore closes by day 26. Neural tube may fail to close due to several factors such as antenatal exposure to drugs like sodium valproate, carbamazepine, trimethadione, aminopterin, thalidomide and alcohol. Other factors associated with neural tube defects include folate deficiency, maternal diabetes, irradiation during pregnancy, hyperthermia and prenatal rubella infection [Figure - 1]. The first trimester screening for malformations needs to be preceded by a pre-test counseling on the need for such screening, what can be the potential outcome of the screening and how we would like to proceed after the screening tests. The protocol for the screening is given in the algorithm [Figure - 2]. All WWE who are using AEDs are advised to take vitamin K 10 mg IM at 34 and 36 weeks of pregnancy. This is because oral vitamin K is not readily available in India. Delivery It is important that delivery is arranged under the supervision of an obstetrician with ready access to neonatologist and physician or neurologist. Care should be taken to ensure that the routine doses of medications are administered to the woman while she is in the labor room. Physical stress, sleep deprivation, hypoglycemia, inappropriate AED dosages and missing dosages and comedications can predispose WWE to seizures during delivery. If required, blood levels of AEDs may be checked to ensure that adequate blood levels are maintained during labor. There should be a plan to handle generalized seizures during labor. Mostly, women can be administered lorazepam 4 mg intravenously if generalized seizures occur during labor. Some of these patients may require cesarean section if they are heavily sedated and are unable to participate in labor. The respiratory efforts can be sluggish in the newborns of WWE, if they were administered much phenobarbitone or other sedating AEDs. A pediatrician should be available to resuscitate the newborn if required. Vitamin K 1 mg IM can be given to the infant to reduce the risk of hemorrhagic disease of newborn. Breast Feeding Breast feeding the baby while using AEDs may have negative impact on child's development. Traces of maternal antiepileptic drugs may find their way into breast milk. The movement of AED into breast milk is inversely proportional to the protein binding property of AEDs [Table - 2]. A recent prospective study showed that there was no difference between infants who were exposed to AEDs through breast milk and those who were not exposed, with regard to the IQ at 3 years of age. [36] It is recommended that mothers first nurse the babies and then consume the AEDs so that the blood levels will not be very high during breast feeding. Frequent interruptions to sleep in order to breast feed the baby can lead to break through seizures in women who were otherwise well controlled. They could use expressed milk to feed the baby during night. WWE are advised to nurse the baby in such a way that in the event of a seizure, they would not drop the baby or fall over the baby and suffocate the baby. Child Rearing Childrearing problems of WWE had been often neglected. WWE may experience considerable stress during postpartum period. They are at higher risk of seizures because of physical exhaustion or sleep deprivation while they wake up frequently to nurse the baby. [37] There is a risk of accidentally dropping the baby during a myoclonus or seizure. Occasionally, WWE are not given an opportunity to attend to their babies. WWE need to be prepared emotionally and physically to handle child rearing efficiently.[39] References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11013t2.jpg] [ni11013f2.jpg] [ni11013t1.jpg] [ni11013f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}