 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
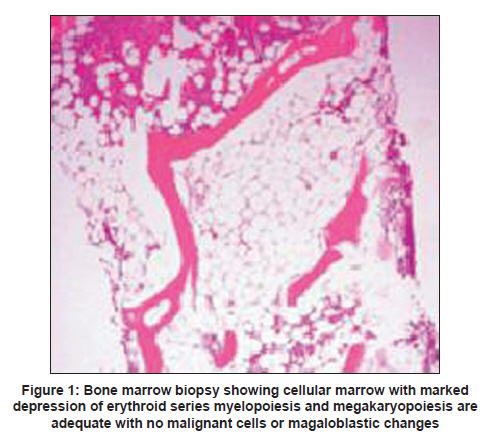
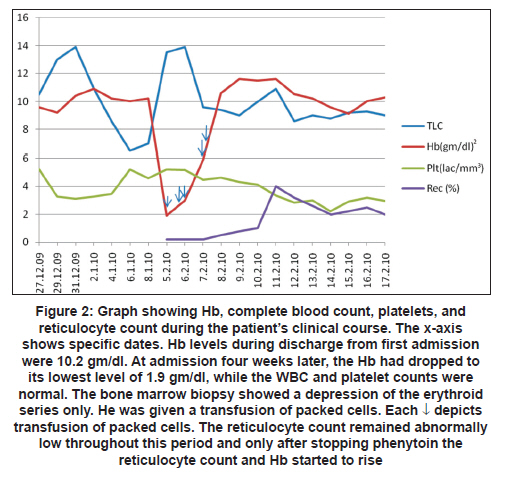
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 69-70 Topic of the Issue: Letter to Editor Pure red cell aplasia with phenytoin following traumatic brain injury G Paul1, P Sood1, A Berry2, BS Paul3 1 Critical Care Division, Dayanand Medical College and Hospital, Ludhiana, India Date of Submission: 28-Apr-2010 Code Number: ni11016 PMID: 21339664 Sir, The hematological, toxic effects of phenytoin therapy are well documented, but drug-induced, pure red cell aplasia is an uncommon disorder. We report the case of acute bone marrow suppression and pure red cell aplasia following prophylactic phenytoin after traumatic brain injury. A 25-year-old male was admitted to Emergency Department after sustaining frontomaxillary injuries His past medical and family history were unremarkable. Neurologic examination showed Glasgow Coma Scale (GCS) score of 13. His hemoglobin was 9.6gm/dl. Computed tomography (CT) of head revealed frontal contusions. He was managed conservatively and discharged about three weeks later on phenytoin anticonvulsant prophylaxis. He was readmitted after one month with complaints of excessive weakness, fatigability, and dyspnea. On examination, significant pallor was noted, with a heart rate of 124/minute and respiratory rate of 30 breaths/minute. Cardiac auscultation revealed a Grade III/VI ejection systolic murmur and a soft S3. Laboratory investigations were: hemoglobulin 1.9 gm/dl; hematocrit 0.565; white blood cell count 13,500/ul, a platelet count of 4.49 lakhs/cumm, and a reticulocyte count of 0.7%. Peripheral blood smear showed moderate anisopoikilocytosis with microcytic hypochromic picture. Chest X-ray and ultrasonography (USG) abdomen were normal and stool for occult blood was also negative. A direct Coombs test was negative and hematinic profile was normal. Liver enzymes were not raised and tests for hepatitis B virus, cytomegalovirus, and parvovirus B19 were all negative. Bone marrow examination [Figure - 1] showed acellular marrow with complete absence of erythropoiesis, adequate myelopoiesis, and megakaryopoiesis, with no malignant cells. Laboratory data supported the diagnosis of pure red cell aplasia. Phenytoin was considered the culprit and was withdrawn. Supportive treatment was given in the form of packed red cell transfusions. The response to phenytoin withdrawal was dramatic, within three weeks hemoglobin increased to 10.5 gm/dl and remained stable thereafter.[Figure - 2] shows the evolution of laboratory data during the clinical course of the patient. Pure red cell aplasia (PRCA) is characterized by severe normochromic normocytic anemia, reticulocytopenia, and isolated erythroblastopenia in the bone marrow, which can be either primary or secondary. Drug-induced PRCA represents an acute and generally reversible form of isolated erythroid aplasia. Of the drugs, only phenytoin, azathioprine, and isoniazid have sufficient evidence of causal association. [1] Our patient had severe anemia, a fall from 9.6 gm/dl to 1.9 gm/dl after starting phenytoin. Hematological workup was suggestive of complete lack of erythropoiesis with normal value of other cell linage. Investigations ruled out other causes of acute bone marrow suppression, thus making phenytoin the most likely culprit. The quick return of counts on discontinuing phenytoin without any specific therapy was consistent with the previous reports of hematological toxicity due to this drug. The association of phenytoin with PRCA has been well-documented. [2] The possible mechanisms of drug-induced PRCA are immune complex damage to the erythroid progenitor cells or beyond the stage of differentiation of the CFU-E, or antibodies against drug-modified antigens on the progenitors. [3] However, the fact that phenytoin is a membrane-active agent and its presence is necessary to induce suppression of erythropoiesis is in favor of its primary role as a hapten. Other possible mechanisms include direct inhibition of DNA synthesis in marrow erythroid cells. [4] The interval between the initiation of therapy and onset of anemia varies widely from four months to four years. [2],[5] Our patients is unique in that the patient developed acute bone marrow suppression and PRCA within one month of phenytoin therapy. The recommended duration of prophylactic anticonvulsant therapy with phenytoin is only seven days in patients with traumatic brain injury. [6] It is prudent on the part of the clinicians to avoid phenytoin therapy beyond the specified period in patients with traumatic brain injury. Patients with drug induced PRCA require supportive care and discontinuation of the offending drugs and treatment of the associated infections. Our patient was managed accordingly. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11016f2.jpg] [ni11016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}