 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
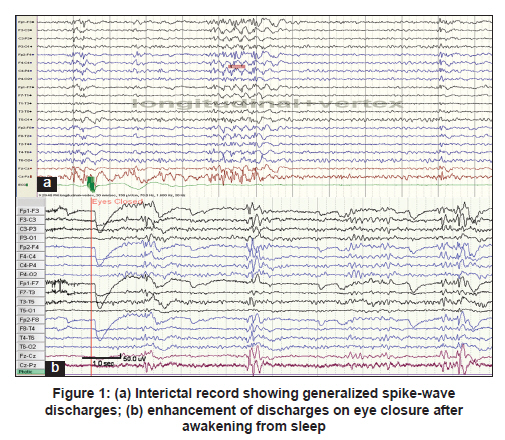
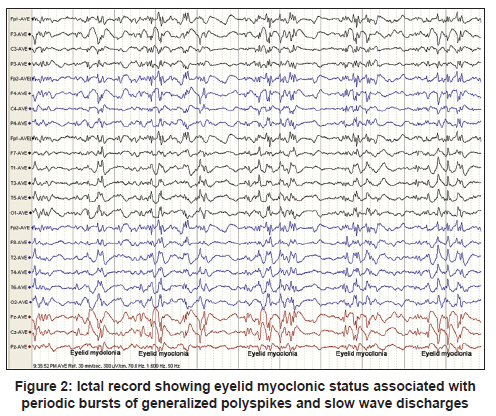
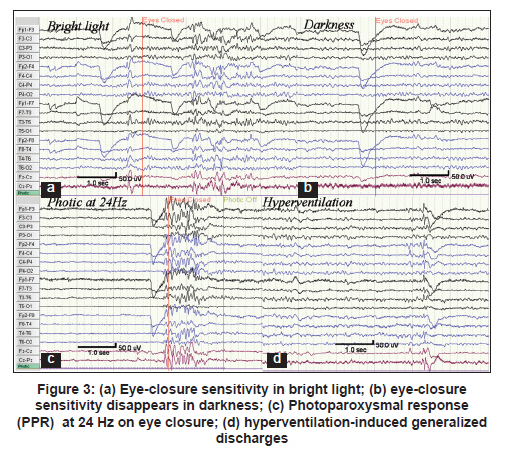
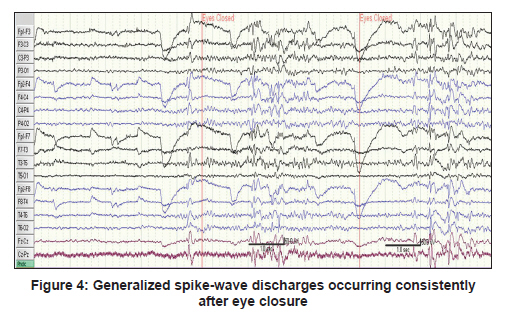
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 70-72 Topic of the Issue: Letter to Editor Oxcarbazepine induced worsening of seizures in Jeavons syndrome: Lessons learnt from an interesting presentation Ramshekhar Menon, Neeraj N Baheti, Ajith Cherian, Rajesh S Iyer Department of Neurology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala, India Date of Submission: 29-May-2010 Code Number: ni11017 PMID: 21339665 Sir, A 19-year-old woman presented with a history of episodic vacant stare with eye blinks and upward deviation of eyeballs since the age of 8 years. From the age of 14 years, she had a few generalized tonic-clonic seizures (GTCS) associated with sleep deprivation. She was initiated on valproate, which was subsequently replaced by lamotrigine. At the time of presentation to us, she was on 5mg/kg of lamotrigine and 20 mg/kg of oxcarbazepine (OXC). Since 1 year before this presentation, she had a run-up of seizures with GTCS occurring every month. Her parents had noted occurrence of eyelid flutter followed by myoclonic jerks involving upper limbs a few seconds prior to these events. On further verification of records, it was noted that the clinical worsening coincided with the initiation of OXC. She did not have history of photosensitivity or family history of seizures. She was found to be normal on cognitive and neurological examination. Further evaluation in the epilepsy-monitoring unit revealed frequent inter-ictal generalized fast polyspikes during wakefulness and sleep [Figure - 1]a. One episode of prolonged eyelid myoclonic status was recorded, which progressed to multifocal myoclonic jerks and GTCS. Electroencephalogram (EEG) ictal accompaniments were generalized 3-6 Hz polyspikes and slow waves [Figure - 2]. In bright light, these discharges occurred consistently within 0.5 to 2 seconds after closing the eyes [Figure - 3]a and [Figure - 4], whereas they disappeared in darkness [Figure - 3]b. These discharges were more frequent on hyperventilation [Figure - 3]d and photic stimulation [Figure - 3]c and on awakening from sleep [Figure - 1]b. Based on the seizure semiology and EEG features, a diagnosis of Jeavons syndrome (JS) worsened by OXC was made. Oxcarbazepine was tapered and levetiracetam initiated. Repeat EEG showed greatly reduced interictal discharges, and at four months follow-up, she reported one episode of brief absence with eyelid myoclonia, on awakening. Jeavons syndrome is a distinct clinical syndrome and the clinical features include eye closure-induced seizures (eyelid myoclonia), photosensitivity, and EEG paroxysms, which may be associated with absence. [1] JS constitutes 2.5% of all epilepsies and 13% of idiopathic generalized epilepsies (IGE). [2],[3] The onset of JS is typically in childhood, peaking at 6 to 8 years. [4] GTCS, though infrequent, is inevitable in adult life, particularly after sleep deprivation, excessive alcohol use or inappropriate use or discontinuation of antiepileptic drugs (AEDs). JS shares many features with juvenile myoclonic epilepsy (JME). The eyelid myoclonus, which is relatively resistant to treatment, is the hallmark of JS; whereas limb myoclonus, which responds well to valproate therapy, is more commonly seen with JME. [5] An AED may paradoxically aggravate epilepsy, predominantly by an inverse pharmacodynamic effect. [6] Oxcarbazepine, like carbamazepine, blocks voltage-gated sodium channels, causing exacerbation of seizures, mainly absences and myoclonus, in IGE. [7] In our patient, the temporal association between initiation of OXC and worsening of seizures, along with the remarkable improvement in the clinical and EEG profile after stopping the drug, strongly supports our diagnosis. Our patient highlights the importance of good history taking as well as the utility of EEG in general and video-EEG in particular, as diagnostic tools in epilepsy. The eye closure manifestations may persist even without photosensitivity, which decreases with age, and hence one should carefully look for it during EEG. Also the eyelid myoclonia once seen can never be forgotten or confused with other syndromes. [2] If the seizure type and syndrome are uncertain, a broad-spectrum AED should be used and AEDs that modulate sodium channels are best avoided in the initial management. A precise syndromic diagnosis is more or less a guarantee against the wrong choice of medication since epileptic syndromes are characterized by specific drug sensitivity. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11017f4.jpg] [ni11017f3.jpg] [ni11017f2.jpg] [ni11017f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}