 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
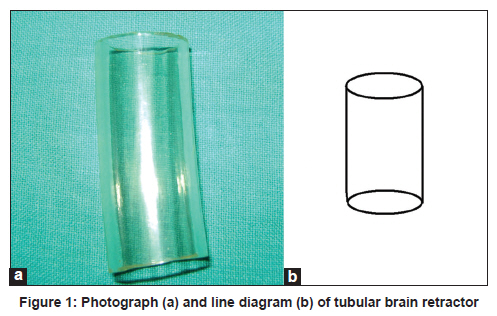
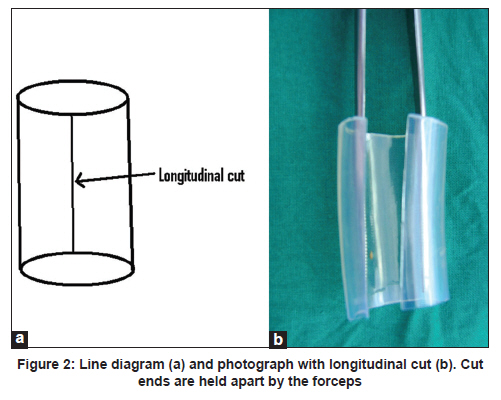
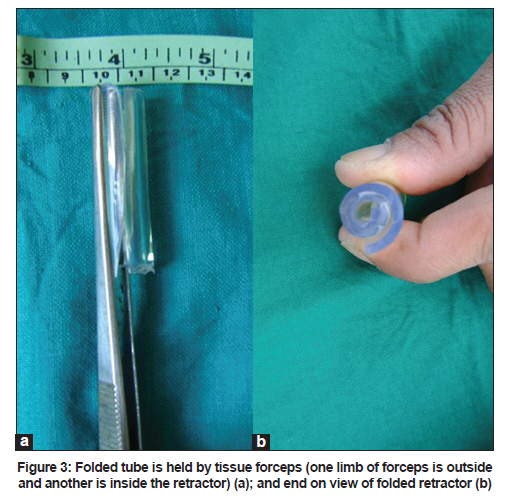
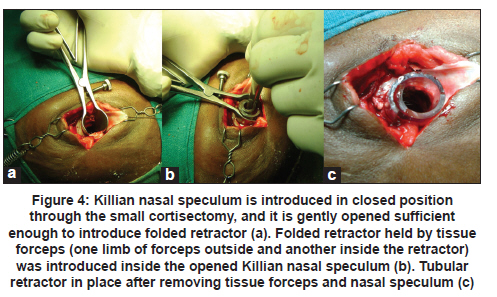
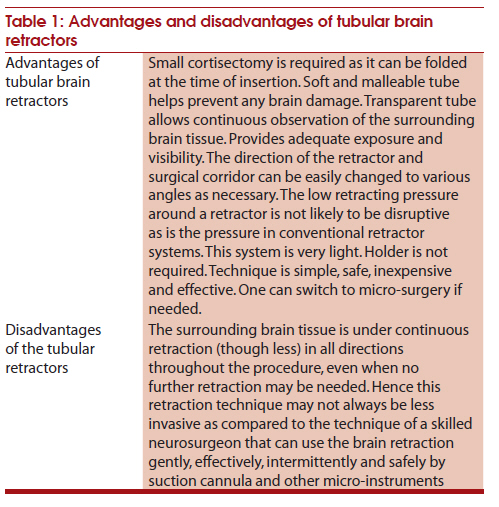
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 74-77 Brief Report A new minimally invasive tubular brain retractor system for surgery of deep intracerebral hematoma Yad R Yadav, Sharda Yadav, Snehal Sherekar, Vijay Parihar Department of Neurosurgery, NSCB Medical College and Apex Hospital, Jabalpur, MP, India Date of Submission: 06-May-2010 Code Number: ni11019 PMID: 21339667 Abstract Access to deep-seated brain lesions with traditional fixed and rigid brain retractors can be difficult without causing significant trauma to the surrounding brain. Tubular retractors offer an advantage of low retracting pressure. We developed a new inexpensive and simple tubular retractor which requires very small cortisectomy. The new tubular retractor was made up of silicone with inner diameter of 15, 18 and 23 mm and outer diameter of 17, 20 and 25 mm, respectively. This tube (1 mm thick) was cut in longitudinal direction. It was folded to make a small-diameter tube so that it could be introduced through a small cortisectomy. Margins of cortisectomy were gently and slowly retracted by Killian nasal speculum. Folded retractor, held by tissue forceps, was introduced inside the opened Killian nasal speculum. Tissue forceps and nasal speculum were removed leaving tubular retractor in place, which comes back to its normal tubular configuration after release. Surgery was performed using rigid Karl Storz 0° telescope (30 cm long and 4 mm in diameter) or microscope. Near-total removals of intracerebral hematomas, 37 hypertensive and 3 traumatic, was done using this retractor without any complication.Keywords: Hypertensive hemorrhage, intracranial hemorrhages, minimally invasive surgical procedures, neuroendoscopy, self-retaining brain retractors Introduction Deep-seated supratentorial intraparenchymal and intraventricular brain lesions can be difficult to access without causing significant trauma to the surrounding brain. Traditional brain retractors use multiple blades, which do not exert equally distributed pressure and thus are traumatic. [1] Complications like hemorrhagic infarct or contusions are reported with the use of such retractors in the region of exposed brain. [2],[3],[4] Most of the present retractor systems are fixed and rigid. Sometimes these retractors create glare in the microscope that distracts the surgeon. Tubular retractors offer an advantage over the conventional retractors. [1],[2],[3],[4],[5],[6] The low retracting pressure around a tubular retractor is not likely to be as disruptive as is the pressure in conventional retractor systems. [7] Although different types of tubular retractors are available, [1],[5],[6],[7],[8],[9],[10] they have their own limitations. We describe a new tubular retractor which is easy to apply, inexpensive, requires small cortisectomy and is safe and effective. Material and Methods This is a prospective study of 40 patients with hypertensive/ traumatic basal ganglionic hematomas with or without intraventricular hematoma treated during a 2-year period from January 2008 to December 2009. The study was approved by the ethics committee of our institute. Written consent was obtained from all the patients or their legal representative. A detailed history, a thorough physical examination and all relevant investigations were performed in all the patients. Hematoma evacuation was done in the initial 10 patients using a microscope with the help of a 23 mm inner diameter tubular retractor. Tubular brain-retractor size was reduced to inner diameter of 18 mm and 15 mm in the next 10 and 20 patients, respectively; and Karl Storz 0° rigid scope 30 cm long and 4 mm in diameter was used to remove the clot in subsequent patients. Patients were evaluated postoperatively by computerized tomography (CT) scan on the first postoperative day in all the patients, and subsequent scans were done as and when needed. Any brain contusion or infarctions and the amount of hematoma removal were recorded. Technique Straight incision of 4-6 cm was made under general anesthesia. Dura mater was opened in circular fashion after reflecting bone flap. The silicone tubular retractors were pre-cut to different sizes of 5, 6, 7 and 8 cm. Sterilized tube of about 30 cm length was also kept ready, and it could be cut to the required size on the table. Small cortisectomy of 6-9 mm was made to reach the hematoma. Part of the clot, which came out spontaneously through the small cortisectomy, was sucked out. Silicone tube with 15, 18 and 23 mm as inner diameter and 17, 20 and 25 mm as outer diameter, respectively, was used as a brain retractor [Figure - 1]a, b. This tube can be obtained from almost all medical instrument manufactures and companies such as Himedia and Tarsons. The tube used was 1 mm thick. It was cut in longitudinal direction [Figure - 2]a and b. It was folded to make a small-diameter tube so that it could be introduced through a small cortisectomy [Figure - 3]a and b. Margins of cortisectomy were gently and slowly retracted by Killian nasal speculum [Figure - 4]a. Folded retractor, held by tissue forceps (one limb of forceps outside and another inside the retractor as shown in [Figure - 3]), was introduced inside the opened Killian nasal speculum [Figure - 4]b. Tissue forceps and nasal speculum were removed leaving tubular retractor in place [Figure - 4]c. Folded retractor comes back to its normal tubular position after release. Its normal tubular configuration can be restored by gentle outward pressure on retractor by two micro-instruments such as suction cannula and dissector. Surgery was performed using microscope or 30 cm long and 4 mm in diameter 0Ί telescope (Karl Storz GmbH and Co.,Tuttlingen, Germany). Telescope with its sheath was then fixed using a holder. Both the hands could be used for evacuation of hematoma with the help of suction cannula, biopsy forceps and other micro-instruments. Bipolar coagulation was used for hemostasis. Proper vision and good magnification were possible in all the cases. Transparent nature of the tube helped in better visualization of the surrounding brain tissue. Bleeding from the cortisectomy margin was controlled while the retractor was gradually withdrawn. This retractor should be autoclaved. It could also be sterilized by activated dialdehyde solution (Cidex solution) or by ethylene oxide (ETO) sterilization. Results A total of 40 patients with hypertensive/ traumatic basal ganglionic hematomas treated during the period from January 2008 to December 2009 were studied using tubular retractor. Re-application, if needed, was equally easy. Follow-up period ranged from 3 to 27 months, with an average of 16 months. Duration of surgery ranged from 60 to 110 minutes, with an average 90 minutes. Near-total removals of hematomas were done in all the patients without any complications such as contusion or infarcts. Discussion Deep lesions can be excised using both microscope and endoscope. Excision of such lesions requires a 2 cms size cortisectomy. Brain tends to fall after removal of the lesion or cerebrospinal fluid (CSF) drainage. The retraction force of conventional brain retractors on the surrounding brain tissue may lead to postoperative neurological injury. A considerable reduction in regional cerebral blood flow with a retraction pressure of 40 mm Hg has been documented. [2] Rosenørn et al.[2] found cortical damage in all the 6 animals studied with brain retraction at a pressure of 40 mm Hg. On the other hand, Ogura et al.[7] found that the retracting pressure around a cylindrical retractor never exceeded 10 mm Hg. This retraction pressure of 10 mm Hg or less does not give rise to any ischemic complications. Although a skilled neurosurgeon can carry out brain retraction effectively by suction cannula and other micro-instruments, yet it is not easy to keep a small cortical window open by forceps and sucker without some kind of retractor. [10] Minimally invasive procedures for intraventricular lesions, including tumors and hematomas, have become popular. [11],[12],[13] Few systems that require small cortisectomy need the aid of a stereotactic or navigation system. [8],[9],[14] All these methods and equipment are very costly and are not available in all neurosurgical centers. Some of the available tubular retractors have their own limitations. [1],[6],[7],[10] Advantage of our retractor is that the cortisectomy required is small. Longitudinal cut reduces outer diameter of our retractor to half at the time of insertion. It is capable to retract even tight brain. The tubular retractor is transparent, lightweight and versatile, can be moved in any direction, avoids time wastage in repositioning and a holder is not required. Soft and malleable tube helps prevent any brain damage. The technique is simple, safe, inexpensive and effective [Table - 1]. One can switch to micro-surgery if needed, although larger-size tube is required as compared to endoscopic technique. The present trans tubular micro endoscopic approach is an alternative to traditional brain retractors and other cylindrical retractors. Limitations of this study are the small number of patients and that it was used in hematoma removal only. Study with large number of patients and its use in tumor excision is required to validate the present study findings. A new tubular retractor system for deep brain lesions is readily available, simple, effective, lightweight and inexpensive. Use of this system minimizes cortisectomy size and avoids retractor-induced trauma to overlying brain. The new retractor with such ease of application seems to be an advantageous alternative compared to the conventional retractors. The tubular retractor is transparent, can be moved in any direction, is versatile and avoids time wastage in repositioning. Our system does not require any holder. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11019f1.jpg] [ni11019f4.jpg] [ni11019f3.jpg] [ni11019f2.jpg] [ni11019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}