 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
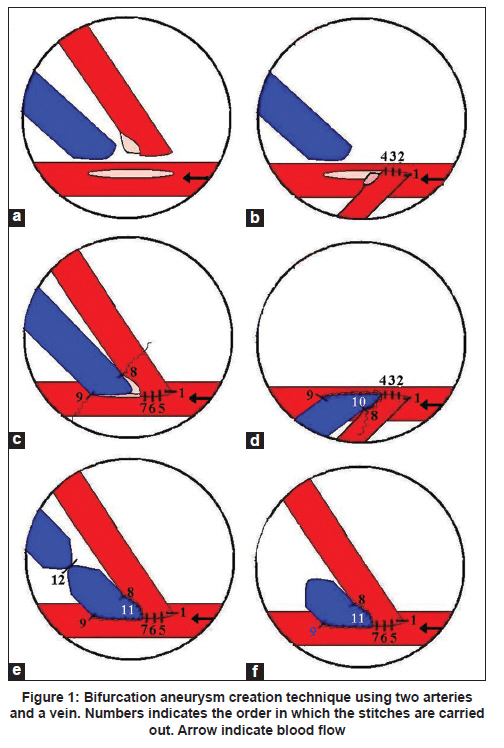
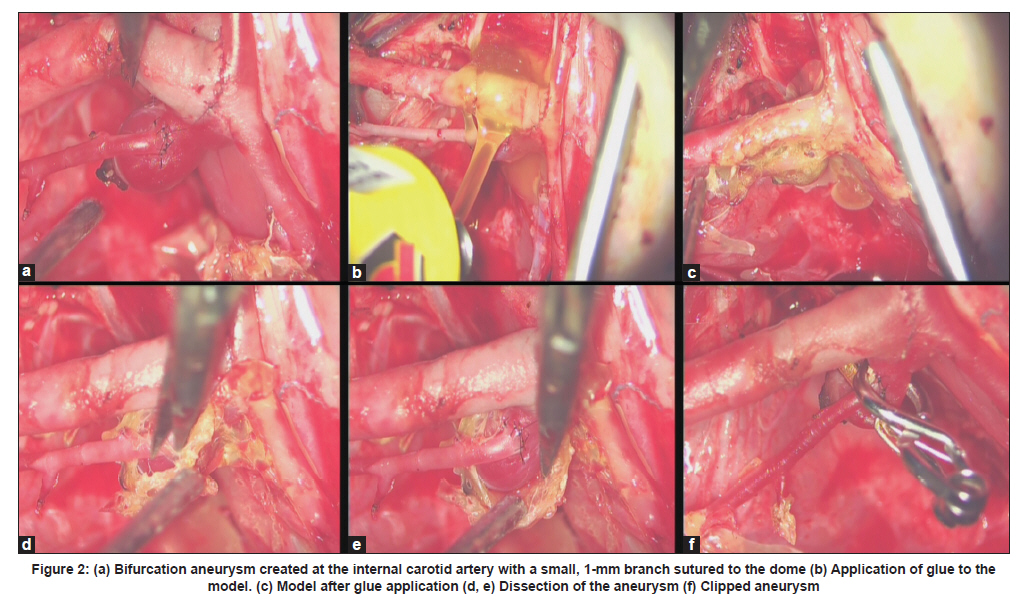
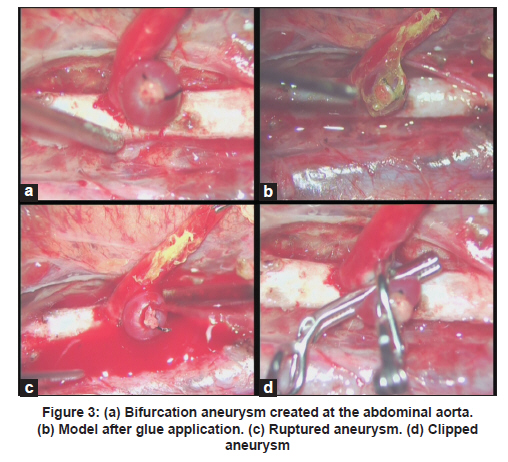
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 78-81 Brief Report Microsurgical cerebral aneurysm training porcine model Jon Olabe1, Javier Olabe1, Jose Roda2 1 Department of Neurosurgery, University Hospital Son Dureta, Palma de Mallorca, Spain Date of Submission: 17-Jun-2010 Code Number: ni11020 PMID: 21339668 Abstract The authors developed a simple reproducible technique for aneurysm creation and adapted it to mimic intracranial dissection conditions using glue application as a pseudo-arachnoid type layer. Ten 1-2-month-old healthy domestic swine were employed under general anesthesia. A novel technique for bifurcation aneurysm creation was developed using two arteries and a vein. After aneurysm creation, diluted sulfuric acid was applied on the dome with a micropipette to increase aneurysm fragility in selected zones. The surgical field was then dried and contact glue was applied around the vascular complex in a circular manner so as to emulate arachnoidal connection fibers. Microsurgical dissection of the aneurysm and surrounding vessels was performed by delicately removing the adhesive substance. Diverse aneurysm clipping techniques, emergency rupture situations and vascular reconstruction procedures were trained. Twenty-two aneurysms were created at several vascular sites, one aneurysm dome ruptured during application of sulfuric acid, two aneurysm models were proved to be thrombosed, two aneurysms ruptured during the dissection and no intraoperative deaths occurred. All aneurysms were clipped in an acceptable manner. This bifurcation aneurysm model provides a novel training system to be used not only by neurosurgeons but also by neurovascular interventionists.Keywords: Aneurysm model, cerebral aneurysm, clipping, endovascular, interventionism, microsurgery, training Introduction Since the International Subarachnoid Aneurysm Trial (ISAT), the proportion of cerebral aneurysms treated microsurgically is decreasing as endovascular techniques are evolving. [1] Straightforward aneurysm morphologies are usually treated with endovascular techniques and only the most intricate ones tend to require microsurgical clipping. [2] Training of these techniques is substantially decreasing by this situation, in which surgical cases decline but are technically more demanding. Aneurysm models have been previously described; however, these were typically used for endovascular training experimentation. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23] The aim of this study was to develop a novel bifurcation aneurysm creation technique simpler than the previous models and adapt it to create a life-like microsurgical aneurysm training system. Material and Methods The experimental protocols used in this study were approved by the appropriate institutional committees on animal welfare and met the guidelines of the European Communities Council Directive 86/609/EEC. Ten 1-2-month-old domestic swine (7-15 kg) were premedicated with ketamine (10 mg/kg IM) and atropine (0.4 mg IM), having been fasted overnight. An intravenous catheter was inserted into the auricular vein for drug administration followed by traqueal intubation with enflurane anesthetic gas. After training, the animals were sacrificed by injecting intravenous potassium chloride solution. Several vascular structures were exposed (using a Zeiss Opmi 1 microscope, Carl Zeiss International S. A., Madrid, Spain) with average diameters of external carotid artery (1.5 mm), internal carotid artery (3 mm), jugular vein (4 mm), infrarenal aorta (6 mm) and lumboradicular arteries (1.5 mm). A novel technique for bifurcation aneurysm creation, whose neck is part of both bifurcated arteries, was developed using two arteries and a vein [Figure - 1] with the use of monofilament 8 cero Ethicon nylon sutures. A large elliptical arteriotomy was performed in the main artery (internal carotid or abdominal aorta). The second artery (either from the carotid artery or previously harvested arteries from the slaughterhouse, cleaned and preserved in glycerine and immersed in heparin solution before grafting) was prepared with a large "fish mouth." A 3-cm segment of jugular vein was extracted and prepared in a standard fashion. The stitching technique starts creating a partial lateroterminal arterial anastomosis with seven interrupted stitches (1-7) between the two arteries, as shown in the figure. Two stitches (8,9) were used to join the vein to the opening of the partial lateroterminal anastomosis followed by closure of both lateral openings with continuous running suture (10,11). The vein was converted into a pouch by transfixion suture (12) and the remaining vessel was resected. The distal arterial clamp was removed soon obtaining backflow and low-pressure filling of the aneurysmal complex. Under high magnification, with only the low-pressure backflow, sharp dissection of the aneurismal venous pouch's adventitia was performed to reduce its mural thickness to minimal. Following this, 20μl of 25% dilute dsulphuric acid were applied at selected zones using a micropipette. The proximal arterial clamp was then removed, obtaining full-pressure blood flow into the aneurysm. In some cases, a 1-2-mm branch of the external carotid artery was anastomosed to the aneurysm in order to complicate the vascular structure's treatment. Aneurysms of different morphologies were created. After aneurysm creation and flow confirmation, the surgical field was dried and glue (PascoΣ contact glue, Pasco fix industrial adhesives, Bayern, Germany) was applied around the vascular complex with the help of a brush in a circular manner so as to emulate arachnoidal connection fibers. The glue was allowed to dry for 10 min. Microsurgical dissection of the aneurysm was performed by removing the adhesive substance [Figure - 2]. Different clipping methods were trained (with Sugita clips), such as tandem or booster, with several clip dispositions and careful verification of correct flow in the parent vessels. Emergency aneurysm rupture situations were caused with proximal vascular control followed by clipping of the ruptured aneurysm and training of diverse reconstruction techniques with sutures. Results Twenty-two aneurysms were created at several vascular sites. Two aneurysm models (9%) were proved to be thrombosed. No intraoperative deaths occurred. One aneurysm model (4.5%) ruptured during application of sulfuric acid to the dome. The average time for model creation, including glue application, was 60 min. Two aneurysms (9%) ruptured during the dissection for glue removal [Figure - 3]. All aneurysm models could be dissected and clipped in an acceptable manner. This process could be repeated by removing the clips and newly applying glue to the model. Dissection of the aneurysm was carried out in a real-like fashion under microscopic vision in order to understand the vascular complex anatomy and design the adequate clipping strategy (see Video 1, Supplementary Digital Content 1, which demonstrates microsurgical aneurysm dissection and clipping). Discussion The aneurysm models are fragile and thus dissection must be carried out in a delicate fashion to avoid dome rupture, especially in selected zones where diluted sulfuric acid has been applied, simulating ruptured aneurysm surgery. The application of glue to the model makes dissection more tedious, imitating the arachnoidal network found in the surgical field. Complete dissection of the vascular complex must be performed before correct understanding of the anatomy followed by clipping manoeuvres and rupture situations resembling cerebrovascular microsurgery. The novel bifurcation aneurysm creation technique is simpler to perform, is less time consuming and is more reproducible than the previous ones described, which involve many complex stitches and result in different aneurysm morphologies. [4],[9],[13],[16],[21] Our model's reproducibility is an important factor, especially for experimental studies of new endovascular devices or techniques. The thrombosis rate of 9% seems adequate. Because porcine models are very thrombogenic, heparin administration should be considered to be added to the model in the future. Future developments of the model are: (1) inclusion of the model in a skull with a craniotomy and simulation of the typical anatomy of the most common aneurysm morphologies and (2) providing some objective evaluation of the claims that this model will aid in neurosurgical education with verification of the model's effectiveness as a training tool. In conclusion at teaching hospitals with low volumes of surgically treated aneurysms, training models will play an increasingly important role in the development of neurosurgical residents. The psychomotor skills used to create the model and the dissection process will familiarize trainees with microsurgical and clip application techniques. However, such models can only supplement and not supplant real-surgery microsurgical experience, where only the transformation from novice to expert can occur. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11020f1.jpg] [ni11020f3.jpg] [ni11020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}