 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
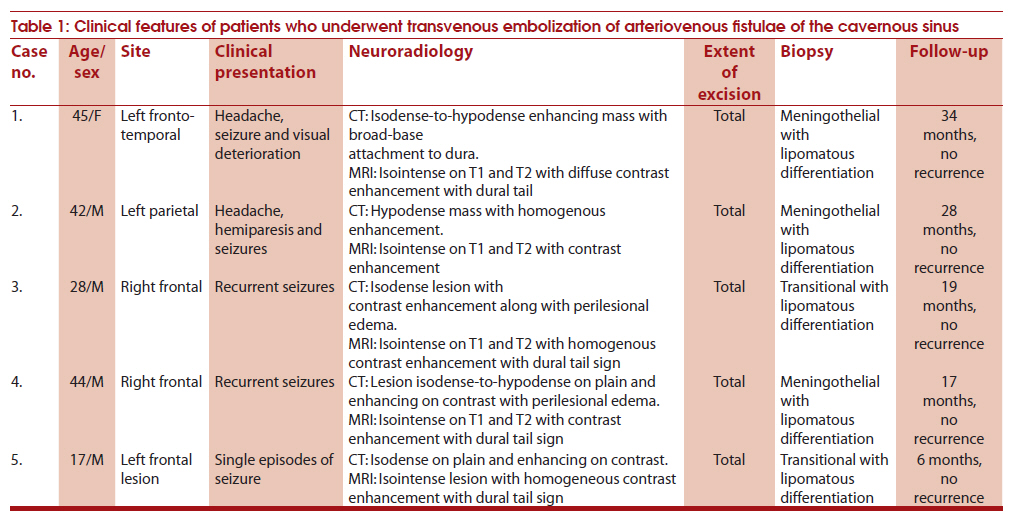
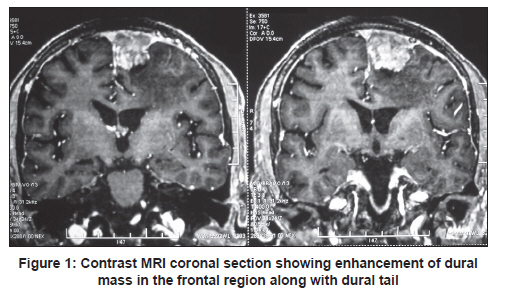
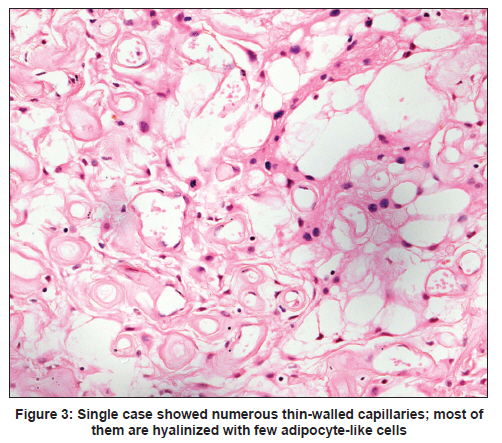
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 87-91 Brief Report Lipomatous meningioma: A study of five cases with brief review of literature Awadhesh Kumar Jaiswal1, Anant Mehrotra1, Brijesh Kumar1, Sushila Jaiswal2, Mukul Vij2, Sanjay Behari1, Lily Pal2 1 Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India Date of Submission: 30-Jun-2010 Code Number: ni11022 PMID: 21339670 Abstract Lipomatous meningiomas are an uncommon subtype of meningiomas. In the present report, the clinical characteristics, neuroimaing and pathological features of 5 patients (4 males, 1 female; age range, 17-45 years; mean age, 35.2 years) with lipomatous meningioma were analyzed. The neuro-pathological reevaluation of lipomatous meningioma involved assessment of histological features proposed by the current WHO classification. The presence or absence of high whorls, fascicles, solid growth, glial invasion, necrosis and nuclear pleomorphism was assessed. The most common presenting symptom was seizures. Location of tumor was frontal (3 cases), parietal (1 case) and fronto-temporal (1 case). All cases showed radiological features of conventional meningioma. Complete excision of tumor along with involved dura was performed in all the patients. Three tumors were meningothelial and 2 were transitional. Tumoral lipid content was variable from 10% to 30%. In addition, there were microcystic features (2 cases) and psammoma bodies (1 case). No recurrence was noted in any of our cases till the last follow-up. Lipomatous meningioma represents a rare distinctive type of meningioma, with a good prognosis with complete removal.Keywords: Lipomatous meningioma, lipomeningioma, meningioma, tumor Introduction Meningioma is a neoplasm of meningothelial cells attached at inner surface of dura mater and it accounts for up to 30% of all intracranial tumors. [1] The terms 'lipomatous' and 'lipoblastic' have been used to designate meningothelial neoplasms containing cells resembling adipocytes or lipoblasts. Bailey and Bucy in 1931 coined the term 'lipomatous meningioma.' [2] Clinical presentation, surgical management and prognosis are similar to those of classical meningiomas. However, histological features are different. Light microscopy of lipomatous meningioma shows focal or widespread mesenchymal adipocyte-like cells (also called lipid-laden cells) admixed with typical meningothelial cells. Thus, it has been considered to be a metaplastic form of meningioma, and it is referenced as so in the World Health Organization (WHO) classification of tumors. [1] However, despite marked histological similarities to the cells encountered in lipoma, the evidence suggests that these tumors result from lipid accumulation within meningothelial cells, rather than an actual transformation to mature adipocytes. [3],[4] The studies on lipomatous meningioma are limited, and only 36 cases have been described in the literature. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17] In this study, we describe the clinical course, neuro-radiological features and morphology of 5 patients with lipomatous meningioma. Material and Methods All evaluable cases of lipomatous meningioma from January 1999 to March 2010 were retrieved from the database files of the Department of Pathology. The clinical, surgical and pathological data of the patients were retrieved from hospital information system, database files of the Department of Neurosurgery and records of the Department of Pathology. Pathological data included tumor location, gross appearance, growth pattern, glial invasion, cellular atypia, mitosis and necrosis. The formalin-fixed paraffin-embedded tissue blocks and tissue sections were retrieved and reviewed. Additional sections of 3-5 ΅ were cut and stained with hematoxylin and eosin. Neuro-pathological reevaluation of lipomatous meningioma involved assessment of histological features proposed by the current WHO classification. The presence or absence of high whorls, fascicles, solid growth, glial invasion, necrosis and nuclear pleomorphism was assessed. Mitotic activity was assessed by counting mitoses in 10 randomly selected high-power fields (HPFs). Results Clinical, radiological and pathological details of 5 patients with lipomatous meningioma seen during the study period are summarized in [Table - 1]. Age ranged from 17 to 45 years, with mean age of 35.2 years and there were 4 males. The most common presenting symptom was seizures. Location of tumor was frontal (3 cases), parietal (1 case) and fronto-temporal (1 case). All tumors were dural. Cerebral edema was evident on imaging in 2 patients. Bone invasion was not seen in any of our patients. All patients showed radiological features of conventional meningioma. On computerized tomography (CT) scan, lesions showed hypodense-to-isodense masses uniformly enhancing on contrast. On magnetic resonance imaging (MRI), these tumors were isointense on T1- and T2-weighted images with homogeneous contrast enhancement [Figure - 1]. Dural tail sign was evident on MRI in 4 patients. The tumors were well circumscribed, extra-axial and clearly separable from adjacent brain. Complete excision of tumors along with involved dura was performed in all the patients. One of the patients developed operative-site extradural hemorrhage in the immediate postoperative period and underwent re-exploration with evacuation of clot. The patient gradually recovered. The postoperative period of all other patients was uneventful. Follow-up ranged from 6 to 34 months, with a mean follow-up of 20.8 months. None of our patients had recurrence till the last follow-up. Three tumors were meningothelial [Figure - 2]a and 2 were transitional. Tumoral lipid content was variable from 10% to 30% [Figure - 2]b. Two tumors showed microcystic features, and psammoma bodies were noted in a single case [Figure - 2]c. The meningothelial cells were predominantly uniform with round-to-oval nuclei and delicate chromatin. The fibrous component showed spindle-shaped cells. In all lesions, lipidized meningothelial cells resembled mature adipocytes with large fat droplet and peripheral displacement of nuclei. Single tumor also contained xanthomatous meningothelial cells admixed with adipocyte-like cells, and a transition between the two components was evident [Figure - 2]d. Three cases showed variably dilated thick-walled vessels. Single case showed numerous thin-walled capillaries; most of them were hyalinized with interspersed islands of round-to-polygonal meningothelial cells [Figure - 3]. One case showed focal area of hemorrhage. Mitotic figures were indiscernible in all cases. No necrosis or atypia was noted in any of our case. Discussion Of the subtypes of meningioma in the WHO classification, meningothelial, fibroblastic and transitional meningiomas are the most common. Other less common subtypes are metaplastic (lipomatous, osseous, chordoid), psammomatous, secretory, angiomatous, lymphoplasmacyte-rich and microcystic meningiomas. According to the WHO classification, all these are slow-growing, benign lesions (grade I). [1] Lipomatous meningioma, also known as lipomeningioma or lipoblastic meningioma, is a rare entity and only 36 cases have been described in the English literature. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17] The largest series included 18 cases [3] and ours is probably the second largest series of lipomatous meningioma. Lipomatous meningiomas represented 0.3% of all meningiomas operated at the Mayo Clinic over 15 years period. [3] Colnat-Coulbois et al. identified only 2 cases of lipomatous meningioma among the 1,642 meningiomas operated from 1989 to 2005, representing 0.001% of the cohort. [4] Most of the reported cases were women, and the median age was above 60 years. [3] However, in our series, of the 5 patients, 4 were males and the median and mean ages were 40 and 35.2 years, respectively. This may reflect a difference in the characteristics of the population in this part of the world or may reflect a chance finding. Clinical presentation of lipomatous meningioma does not differ from that of the other types of meningiomas and depends on the location of the tumor and the presence of peritumoral edema. Seizures and headaches are the most common symptoms at diagnosis. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17] Seizures were the most common presentation in the present series. Most of the reported tumors occur in supratentorial location. The series by Roncaroli et al. also reported 2 spinal cases. [3] Radiological features of lipomatous meningioma depend on the amount of fat accumulation inside the tumor. When the fat component is predominant, the tumor presents characteristic radiological appearance of low density on CT scan and hyperintense signal on T1- and T2-weighted MRI sequences. [3],[4],[8],[15],[16],[18] On fat suppression sequence, there is signal loss. Contrast enhancement is the rule. Areas with attenuation coefficient of −50 to −100 HU indicate the presence of fat. Intracranial lesions that present areas with such attenuation coefficient are lipomas; dermoid cysts; and the two forms of meningioma, lipoblastic and xanthomatous. However, lipomas and dermoid cysts do not have any meningeal components (dural attachment with dural and osseous reactions). [19] Lipomas usually present as homogeneous expansive lesions of well-defined limits and are located in the midline. Dermoid cysts or teratomas are heterogeneous lesions with solid areas intermingled with areas with an attenuation coefficient similar to that of fat and, possibly, with rough calcifications, and are also located in the midline. Lipid storage also occurs within some malignant tumors, such as metastatic mucinous carcinomas, pleomorphic xanthoastrocytomas and some glioblastomas. When the fat component is less, heterogeneous signal on T1- and T2-weighted MRI sequences is observed. [3] All cases in our series showed radiological features of conventional meningioma. On CT scan, lesions showed hypodense to isodense masses enhancing on contrast. On MRI, these tumors were isointense on T1- and T2-weighted images with homogeneous contrast enhancement. It was because the fat component was not predominant in our cases. The pathogenesis of lipomatous meningioma remains poorly understood. The 2007 WHO classification of the tumors of the nervous system has included these within the metaplastic meningioma group. By definition, metaplasia is a reversible change in which one adult cell type is replaced by another adult cell type. This may represent an adaptive substitution of cells. This implies that arachnoidal cap cells, from which meningiomas arise, may undergo gradual transformation into other cell types such as fat, bone, cartilage and myxoid tissue. The process of metaplasia implies full expression of the characteristics of such "new" cells. On the contrary, occasional ultrastructural studies of lipomatous meningioma have shown that lipid-laden cells retained meningothelial characteristics such as those of desmosomes and lacked specific features of adipocytes. So the adipocytic tissue in lipomatous meningioma is short of true metaplasia. It has been suggested that lipomatous meningioma should no longer be considered as a metaplasia and that lipid accumulation results from a metabolic abnormality of the neoplastic cells. Pathological analysis shows that most of the lipomatous meningiomas are of transitional or fibroblastic type. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17] Two examples of secretory type have also been reported. The prognosis is good provided that removal is complete. Recurrences after surgery have been described in 3 cases, but resection was incomplete in all the 3 cases. [3] Two cases of atypical lipomatous meningioma have also been reported. However, follow-up in these 2 cases is too short to establish a prognosis. [3] On analysis, light microscopy of lipomatous meningioma typically shows two apparently different populations of cells - meningothelial cells and lipid-laden cells. The cytoplasm is filled with a large fat droplet, and the nucleus is placed peripherally. The second type of fat deposition is seen in the xanthomatous variant. There are cells containing numerous fine vacuoles of fat, with a centrally located nucleus. It has also been suggested that lipomatous and lipoblastic features are the result of metaplastic change and that xanthomatous change is simply due to lipid storage. However, both the cells were identified in our single case. Roncaroli et al. also showed cell transitions between xanthomatous and lipomatous forms in one of their cases, which raises some doubts about these distinctions. One of our cases showed numerous venules and capillaries with hyalinized wall and degenerative atypia in meningothelial tumor cells. On extensive review, only 1 case with combined lipoangiomatous features has been reported in literature. [6] The differential diagnosis of these tumors includes vascular malformations and capillary hemangioblastoma. Some meningiomas, particularly microcystic meningioma and clear cell meningioma, are also included in the differential diagnosis of lipomatous meningioma. Microcystic meningioma is characterized by cells with thin elongate processes encompassing microcysts containing pale eosinophilic mucinous fluid. Clear cell meningioma is patternless and composed of round-to-polygonal cells with glycogen-rich clear cytoplasm and prominent stromal and perivascular collagen. [1] Clear cell meningioma is important as it is an aggressive tumor with frequent recurrence and occasional cerebrospinal fluid (CSF) seeding. [1] Although all the fat-containing meningiomas behave as ordinary meningiomas, the reason for the rapid progression of symptoms in reported cases is probably related to development of the surrounding edema, which is unrelated to fatty degeneration. Differentiation of the lipid-containing meningioma from malignant entities is of paramount importance because their treatment modalities are different from those for meningiomas. Conclusions A series of 5 cases of lipomatous meningioma with reference to their clinical, radiological and pathological features is presented. They represent a rare distinctive type of meningioma, with a good prognosis after complete removal. Their clinical features are similar to those of conventional meningioma; however, their radiological features depend on the amount of fat component in the tumor. It may also be suggested that it is more appropriate to consider this type as a lipidized meningioma rather than a true metaplasia. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11022f2.jpg] [ni11022t1.jpg] [ni11022f1.jpg] [ni11022f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
![[Figure - 2]](/showimage?ni/photo/ni11022f2.jpg){kind=link}
{kind=link}