 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
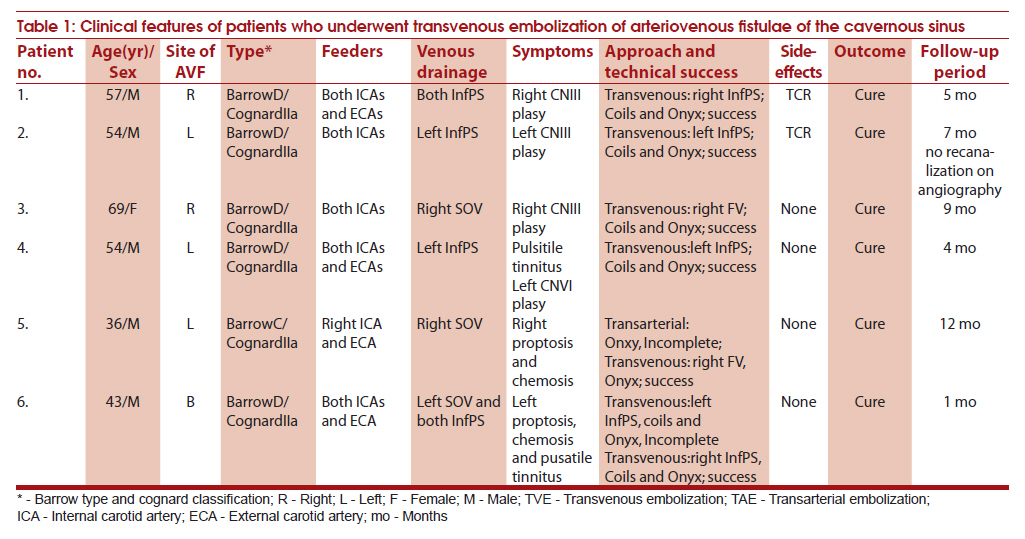
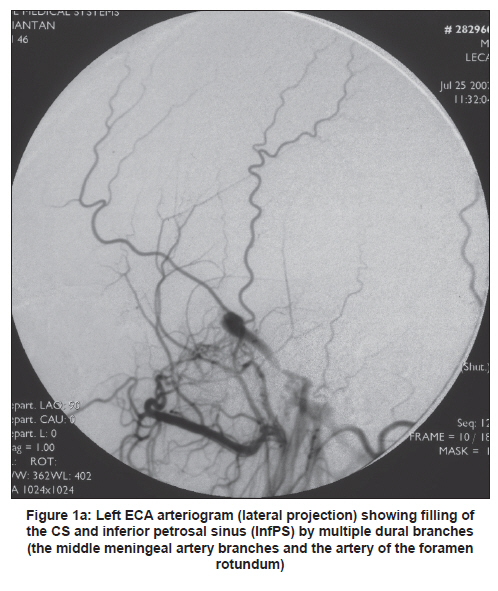
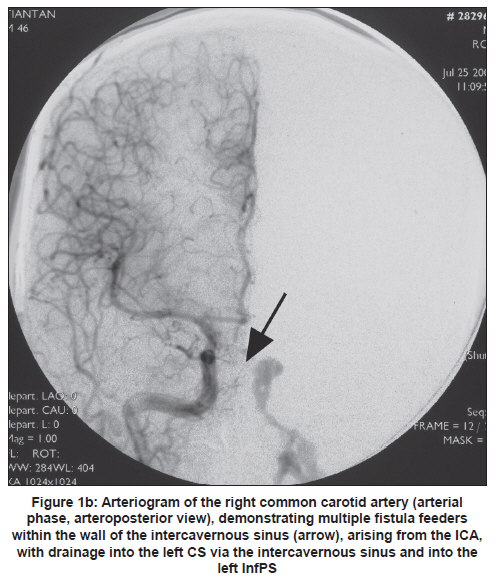
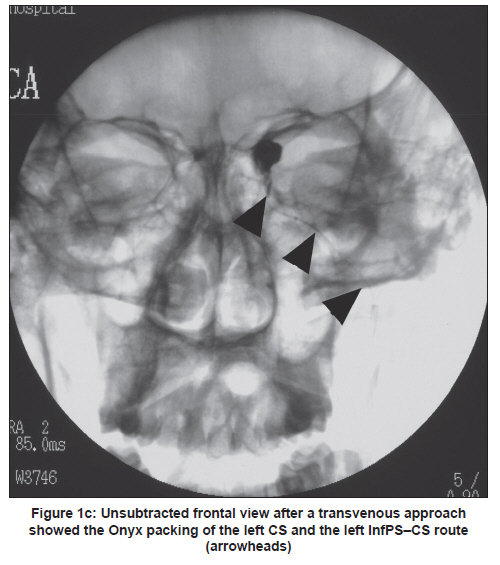
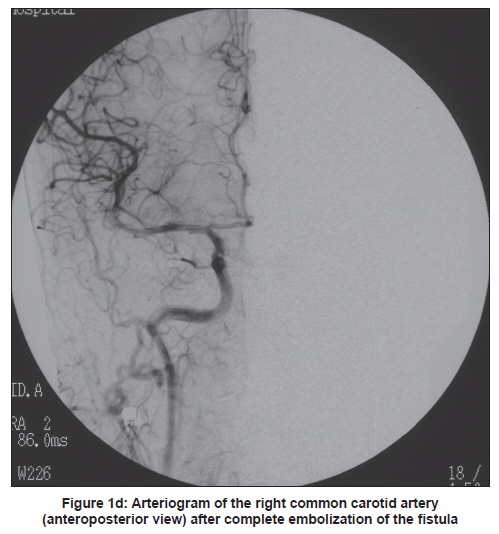
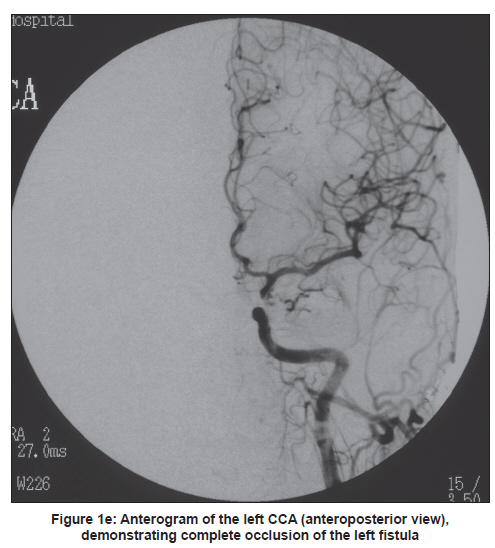
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 92-96 Brief Report Transvenous treatment of complex cavernous dural arteriovenous fistulae with Onyx and coils Liang Li, Jin-guo Cui, Zhi-hui Liang, Shu-bin Xu, Jia Li, Hui-qin Tian, Yu-hong Fan Radiology Department, Bethune International Peace Hospital, Shijiazhuang, Hebei Province, China Date of Submission: 24-Feb-2010 Code Number: ni11023 PMID: 21339671 Abstract Transvenous embolization has become the treatment of choice for such lesions We evaluated Onxy for patients with cavernous dural arteriovenous fistulae (CDAVFs) who underwent transvenous embolization via different transvenous approaches. Case records of six patients with symptomatic CDAVFs, treated between October 2006 and November 2007 were reviewed. A total of seven transvenous procedures were performed in the six patients with CDAVFs. All the patients with CDAVFs of the cavernous sinus were symptom free following embolization. The approach via the internal jugular vein and the inferior petrosal sinus was possible in four of the six patients, with complete occlusion of the fistula. In the remaining two patients, the approach was via the facial vein. Transient bradyarrythmia without morbidity was the only complication in two patients.Keywords: Arteriovenous fistula, cavernous sinus, dural arteriovenous malformation, transvenous embolization Introduction The decision to treat carotid cavernous fistulae (CCFs) is based on several factors: pattern of venous drainage, natural history of the lesion, severity of presenting symptoms, age and general condition of the patient, angiographic characteristics (number and location of feeders, location of dural arteriovenous fistulae DAVFs), and the procedure related morbidity and mortality rates. [1] Treatment goals include obliteration of the fistulae and relief from the symptoms. Treatment modalities of cavernous dural arteriovenous fistulae (CDAVFs) include: endovascular procedures with transvenous, transarterial or transarterial-transfistulous embolization, [2],[3],[4],[5],[6] surgery to access the fistula for embolization either on the venous or the arterial side or to excise the fistula, [7],[8],[9] gamma knife surgery [10] or combinations of any of the three. [4],[11],[12] Some lesions may require only conservative treatment. [13] Because of frequent recanalization and low cure rates, [6] transarterial embolization is limited to Barrow type C fistulae and Barrow Type D fistulae. Transvenous embolization has become the treatment of choice for such lesions. [5],[14],[15] In this article, we evaluated the efficacy and safety of different transvenous embolization techniques for the treatment of CDAVFs, with an emphasis on the use of Onyx via different transvenous routes. Patients and Methods The case records of six patients with CDAVFs treated between October 2006 and November 2007, via different endovascular transvenous routes, were retrospectively analyzed. The data are presented in [Table - 1]. Bilateral selective internal carotid artery (ICA) and external carotid artery (ECA ) angiography and vertebral artery angiography were performed in all the patients to assess the feeding arteries, fistula sites and venous drainage. The arteriovenous malformations were approached via the venous route. We first placed 6-French sheaths in the femoral artery and vein. A 5-French catheter in the carotid artery allowed observation of the shunt, acquisition of roadmaps and angiographic monitoring of the procedure. A second 5-French guiding catheter was positioned in the jugular vein. A microcatheter (Echelon10/Marathon, MTI-EV3, Irvine, CA, USA) was navigated coaxially via different venous approaches. The microguiderwire (Silverspeed10/Mirage, MTI-EV3, Irvine) was then carefully introduced and advanced into the cavernous portion, followed by the microcatheter. All embolizations were performed with Onyx or combined with detachable coils using real-time digital subtraction fluoroscopic mapping. Six patients (one female and five male patients; age range, 36-69 years, mean age, 52.3 years) presented with spontaneous DAVFs of the CS of Barrow Types C to D (Type C, n = 1; Type D, n = 5). Neurologic findings included third cranial nerve palsy in 3, exophthalmos in 2, chemosis in 2, pulsatile tinnitus in 2 and sixth cranial palsy in 1. All the six AVFs of CS were Type IIa. [16] The clinical follow-up periods after endovascular treatment ranged from 1 to 13 months (mean, 7.3 months). Results Transvenous embolization of the CS A total of seven transvenous approaches were performed in the six patients with AVFs of the CS. The data are summarized in [Table - 1]. Of the five patients with Barrow Type D fistulae, one was treated initially via the transarterial approach and subsequently via the transvenous route. Other patients with CDAVFs were initially teated via the transvenous route. If the drainage was predominant posteriorly, the approach was via the internal jugular vein (IJV)-inferior petrosal sinus (InfPS)-CS (n = 4). If the InfPS could be passed (n = 4), then the success rate was high, with complete occlusion in four patients. The transvenous approach via the facial vein (FV) exhibited technical success; complete occlusion of the fistula was possible in the two patients. All the six patients with DAVFs of the CS had relief of clinical symptoms. Two patients had , transient bradycardia related to dimethyl sulfoxide (DMSO) injection. However, there was no permanent morbidity related to this event. Illustrative case Patient 4 A 54-year-old man presented with left sixth cranial nerve palsy and left pulsatile tinnitus. Cerebral angiogram showed Barrow Type D/Cognard Type IIa DAVF, with drainage into both CSs and, predominantly, the inferior petrosal sinus on the left side [Figure - 1a and Figure - 1b]. There were multiple feeders arising from both the ICAs and the ECAs. Because of opacification of the left InfPS, this approach was chosen. Packing of the left CS with coils and Onyx occluded the fistula. Control angiography performed on both sides demonstrated complete occlusion of the fistula [Figure - 1c and Figure - 1d and Figure - 1e]. The VIth cranial nerve palsy improved the following day. Discussion For sequential occlusion and for planning of the venous approach, the drainage system of DAVFs must be carefully analyzed with respect to the drainage of the brain and anatomic variants. [5] When catheterization is possible, transvenous embolization is associated with a high rate of permanent long-term occlusion. [16],[17] Occlusion can be achieved with placement of coils, via a trans-sinusoidal route, in the venous channel of a DAVF outside the sinus lumen [5],[14],[18],[19] or occlusion of the involved sinus segment. We have used a new liquid embolic agent (Onyx) for embolization of dural fistulas of the cavernous sinus. Its nonadhesive and cohesive properties make this agent suitable for transvenous casting of the cavernous sinus. [8],[20],[21] The Guglielmi detachable coils (GDC) are more expensive and less thromobogenic than the platinum mirocoils. To achieve complete occlusion, the cavernous sinus was tightly packed with GDCs. This tight packing may account for the intense nausea, vomiting and third or sixth cranial nerve palsy following coil embolization. [22],[23] However, our patients did not develop a new cranial nerve palsy. There was no recanalization at 7-month control grams, and the embolic agent was safe and permanent. In our patients, inappropriate occlusion of the draining vein did not occur and we achieved a good clinical outcome. From this point of view, we prefer to use platinum coils and Onyx because of their radiological opacity and controllable characteristics. Detachable platinum coils and Onyx-34 were used during the venous approach in case of high-flow cavernous DAVFs. Onyx injection was performed into a basket of coils. In this situation, distal migration of glue to the ophthalmic vein can be avoided. If the tip of the microcatheter reached the fistula point, Onyx injection can also be performed without delivery of platinum coils. If Onyx migration was found under biplane roadmapping, the injection was stopped, waiting for the solidification of Onyx. Then, the injection was continued to pack the cavernous sinus. The complex nature of the fistula, the unexpected hardship in the placement of detachable coils and our previous experience with Onyx in the treatment of DAVFs promoted us to use Onyx in the treatment of our patient. [8],[20],[21],[24],[25] The slow injection of the agent might have been the key factor that enabled gradual casting of the sinus, with filling of its interstices and blocking of the minute fistulous communications. During the intracavernous injection of the embolic agent, caution was exerted to avoid inadvertent embolization of the left internal carotid artery during the slow injection of Onyx. Reflex bradycardia occurred in two patients. This was blocked with atropine, and did not recur. Trigemocardiac reflex may be related to irritation of the trigeminal ganglion or afferent fibers within the cavernous sinus, respectively, by DMSO injection, Onyx formation or sudden change in venous hemodynamics during the embolization procedure. Specifically, as the reflex occurred during the initial phase of our transvenous embolization, it is unlikely that the Onyx mass itself compressed the division of the trigeminal nerve. [26] It is most likely that some sort of chemical irritation might have resulted. The other concern could have been the potential neurotoxity of DMSO on the trigeminal cranial nerve within the cavernous sinus. We speculate that a slow rate of injection may give DMSO enough time to dissipate in the blood stream, and may prevent the toxic effects. [8],[20],[21] References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11023f1c.jpg] [ni11023f1a.jpg] [ni11023f1e.jpg] [ni11023f1d.jpg] [ni11023f1b.jpg] [ni11023t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}