 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
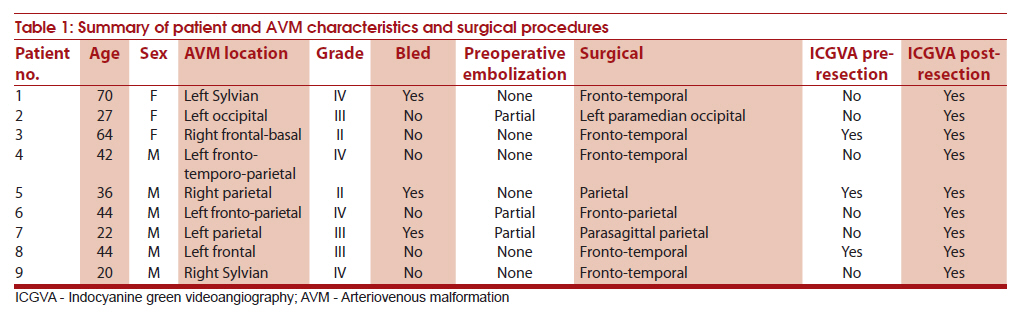
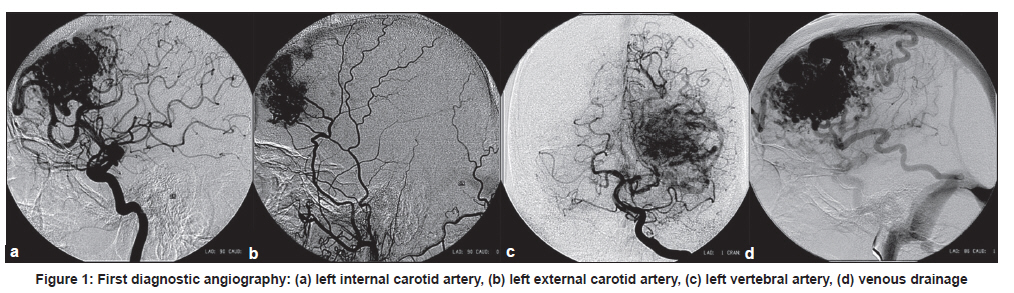
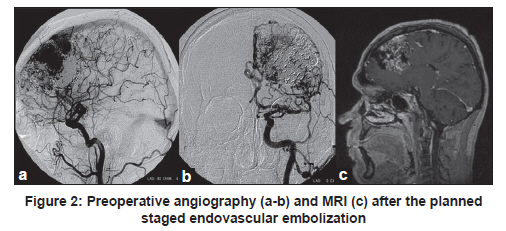
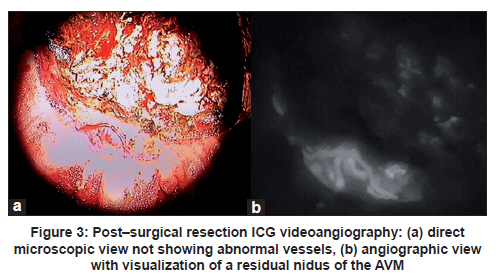
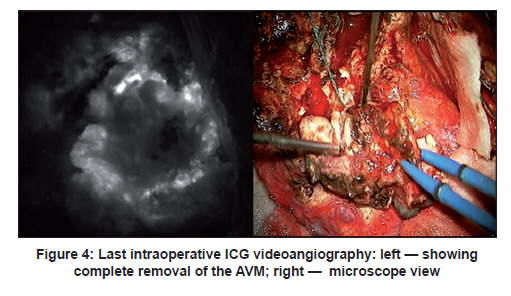
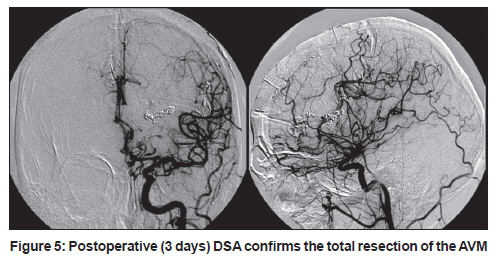
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 97-100 Brief Report Arteriovenous malformations and intraoperative indocyanine green videoangiography: Preliminary experience Graziano Taddei1, Claudio De Tommasi2, Alessandro Ricci2, Renato J Galzio3 1 University of L'Aquila, Department of Health Science, Italy Keywords: Arteriovenous malformation, digital subtraction angiography, indocyanine green, surgical microscope Introduction Fluorescence angiography has recently elicited much interest for the assessment of the vascular anatomy during neurovascular procedures. [1],[2],[3],[4] Since late 1960s, Feindel demonstrated its usefulness in the visualization of cerebral vertebral arteries during surgical procedures. [5] Intraoperative indocyanine green (ICG) videoangiography was first used by Raabe for aneurysm surgery. [2],[3] Woitzik also showed its efficacy during extracranial/intracranial bypass surgery, and Takagi verified the ability of this technique to detect a residual nidus of an arteriovenous malformation (AVM). [6],[7] ICG is a near-infrared (NIR) fluorescent tricarbocyanine dye approved by the US FDA to evaluate cardiovascular and liver functions in 1956; and for ophthalmic angiography, in 1975. [1],[2] After intravenous injection, it binds almost completely to globulin, so the dye remains intravascular with a normal vascular permeability. ICG is not metabolized, has a plasma half-life of 3 to 4 minutes, and it is excreted exclusively by liver without entering the entero-hepatic circulation. The dye is injected into peripheral vein as a bolus, [2] and the operative field is illuminated by an NIR light. As soon as the dye solution arrives in the operative field, ICG fluorescence is induced and recorded by a video camera through an optical filter blocking both ambient and excitation light. [2],[3],[8] We use the Carl Zeiss OPMI Pentero (Oberkochen, Germany), which integrates the microscope with ICG videoangiography technology. The technical integration is described elsewhere. [3],[8] The aim of the present study was to assess the usefulness of ICG videoangiography in the treatment of AVMs and to compare the intraoperative findings with those of early postoperative DSA. Material and Methods Since October 2007, the technique is being utilized during all vascular surgical procedures. We included in the present study patients with AVMs: 3 women and 6 men (age range, 20-70 years; mean, 41 years). AVMs were classified according to Spetzler-Martin grading system. [9] The characteristics of the patients, the location of the AVM and the surgical approach are detailed in [Table - 1]. Among these patients, according to the grade of the AVM and the clinical findings, 3 patients were treated with preoperative embolization. All patients were interviewed regarding history of iodine allergy or previous anaphylactic reactions to contrast media or dye injections, and written informed consent was obtained to perform ICG videoangiography during AVM surgery. ICG videoangiography was performed during all the 9 surgical procedures. The standard dose of 25 mg of ICG for each injection was used in all cases. The setup allowed seeing on the integrated microscope video screen, in real time, high-resolution and high-contrast NIR angiographic images; saving them on internal hard disk; and replaying them if necessary. The technique was planned to be used before and after the surgical resection of the AVM to confirm the total obliteration and removal of the anomalous vessels. Furthermore, if necessary, videoangiographic study was repeated three times in each patient, within 15 minutes following clearance of ICG, without problems with regard to patient safety and image quality. Results During the 9 surgical procedures, 16 intraoperative ICG videoangiographies were performed. After the intravenous injection of the fluorescent dye, with a latency of approximately 10 seconds, a clear contrast enhancement of the vascular system was obtained, accentuating the angioarchitecture (such as feeders, nidus, transit arteries, and venous drainage) and hemodynamic peculiarities of each AVM. In 3 patients with grade II AVMs, the microscope-integrated ICG videoangiography was used twice, before and after the resection of the nidus of the AVM. In 4 patients with grade III or more AVMs, ICG was used only once, viz., after the resection of the nidus, and it confirmed in all the patients total removal of the lesion. In 2 patients with grade III AVM, this technique was used twice and four times, respectively, and the surgeon was able to perform surgery during the intraoperative ICG angiography and to directly verify the effectiveness of his maneuvers. In all these patients, the total resection of the abnormal vascular malformation was confirmed. In Patient 6, the intraoperative ICG evidenced a residual nidus and enabled its total resection during the same surgical procedure. In all the patients, postoperative DSA confirmed the intraoperative ICG findings, that no residual malformations were present. We did not encounter side effects or postoperative complications due to ICG dyein our series. Illustrative case Patient 6 A 44-year-old man with persisting headaches went through neuroradiological assessment. Cranial computer tomography (CT) scan and angiography documented the presence of voluminous left fronto-parietal AVM (Spetzler-Martin grade IV) [Figure - 1]. The patient underwent planned staged embolization of the AVM. Three endovascular procedures were performed for obtaining a final partial obliteration (70%) [Figure - 2], but neither the nidus nor the venous drainage presented definitive modifications in the angioarchitecture. The patient underwent surgical procedure through a left fronto-parietal approach, and intraoperative ICG videoangiography was performed after the surgical resection of the nidus to evaluate the effective removal of all the pathological vessels. This technique allowed the surgeon to identify a residual of the nidus that was not possible to visualize under the direct microscopic view [Figure - 3]a but was demonstrated to be abnormal under ICG angiographic view [Figure - 3]b. Therefore, a further resection of the nidus was performed, and consequently the ICG videoangiography showed total removal of the AVM [Figure - 4]. The patient exhibited no deficits after surgery, and early postoperative DSA (3 days post operation) confirmed the total removal of the lesion [Figure - 5]. Discussion On the basis of our preliminary clinical experience, we confirm that ICG videoangiography is a helpful tool for performing surgery for AVMs. [2],[10],[11] Compared to grade I-II AVMs, we have noticed that in case of large AVMs, grade III-IV, a pre-removal ICG videoangiography does not really help the surgeon to understand the angioarchitecture of AVMs because the superficial anomalous vessels interfere with the view of the deeper portion of the nidus, making difficult the direct verification of the entire three-dimensional structure of the AVMs. So we preferred to perform only a post-removal ICG videoangiography in these cases. Moreover, it is possible to perform surgical maneuvers under the fluorescent view so as to better identify and remove the malformed vessels. Postoperative DSA is the standard method to assess the anatomic results of vascular neurosurgical procedures, but an additional surgical procedure is required when an abnormal finding is noted. [2],[3] Intraoperative DSA could be used in complex cases, with significant effects on the surgical procedure in 7% to 34% of cases. [7],[12],[13],[14],[15],[16],[17] However, it is technically demanding, expensive and requires additional time and human resources. [11],[14],[18] Conversely intraoperative ICG videoangiography is available for all patients within 2 minutes, and there is no need to interrupt the operation or to move the microscope away from the surgical field. The major reported limitation of the microscope-integrated ICG videoangiography is that the angiographic views are restricted to the angle of the surgical approach, and vessels covered by blood clots or brain tissue cannot be observed with this technique. [3] Except for this limitation, the ICG videoangiography gives us the opportunity to analyze with high accuracy the surgical field after the removal of the nidus to confirm the result and to detect an eventual residual of AVM, as reported in the illustrative case. It represents an easy-to-use, cost-effective technique that is safe for patients, as demonstrated by its rates of adverse reactions when compared with those of the other types of contrast media. [19],[20] References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11024f5.jpg] [ni11024f4.jpg] [ni11024f1.jpg] [ni11024t1.jpg] [ni11024f3.jpg] [ni11024f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}