 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
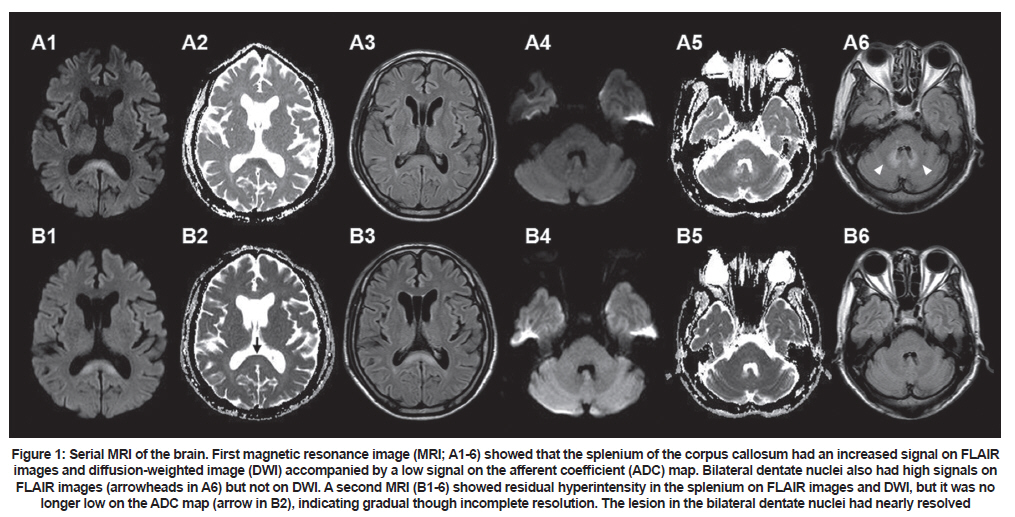
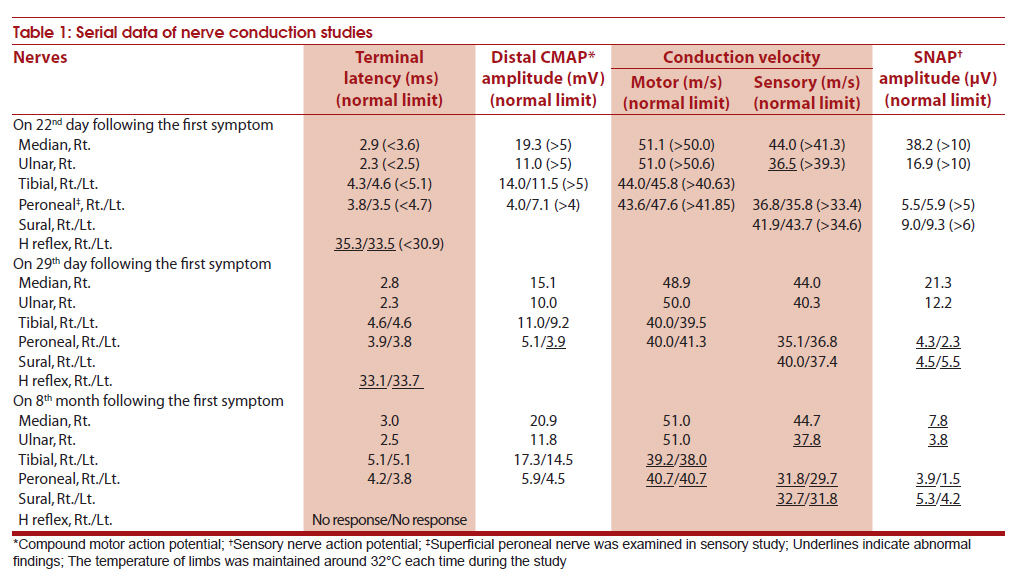
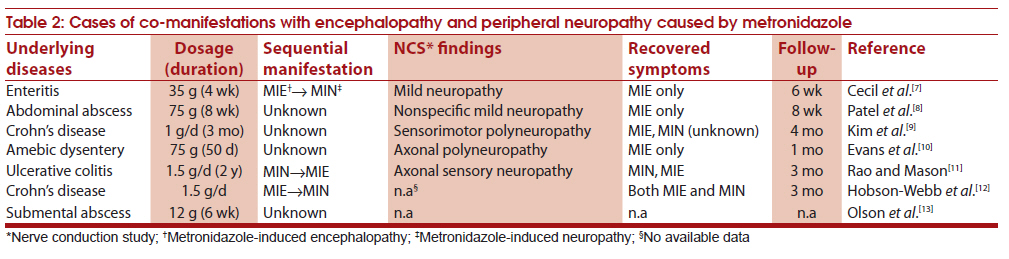
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 104-107 Case Report Metronidazole neurotoxicity: Sequential neuroaxis involvement Kyung-Il Park, Jae-Myun Chung, Ji-Young Kim Department of Neurology, Seoul Paik Hospital, Inje University College of Medicine, Jur-dong, Chung-ku, Seoul, Korea Keywords: Autonomic nervous system, metronidazole, sequential neurotoxicity Introduction Metronidazole is a nitroimidazole mainly effective against anaerobes. The neurotoxicity of metronidazole is dose-related and includes polyneuropathy and encephalopathy. [1],[2],[3],[4],[5],[6],[7],[8],[9] However, sequential involvement of peripheral, central and autonomic nervous systems have not been reported. We report one such case with imaging and neurophysiologic studies. Case Report A 67-year-old man was admitted for the evaluation of paresthesias and pains involving the legs and hands. Ten weeks before this admission he was treated for hepatic abscess with cefotaxime (6 g parenterally per day) and metronidazole (500 mg three times per day parenterally) for 3 weeks, which was subsequently then changed to cefixime (200 mg per day) and metronidazole (500 mg three times a day per orally). Total cumulative dose of metronidazole at this point was 75 g. He developed paresthesias and pains in both the feet, three weeks before this admission to our hospital. After 10 days of onset of paresthesias and pains in the lower limbs, the symptoms further progressed to the level of the knees. On admission, the paresthesias were found to involve both hands. There was no history of prior infections or alcohol consumption. Vitals were normal. On neurological examination he was alert and well oriented. Cranial nerve and motor system examination was normal. Deep tendon reflexes: bilateral knee, ankle and biceps were absent with plantar flexor response. He had loss of pinprick sensation below the knees and position sensation at toes. Complete blood picture and routine blood biochemistry were normal. Serology for human immunodeficiency virus, hepatitis B and C virus and syphilis were negative. Cerebrospinal fluid examination was normal. A nerve conduction study (NCS) revealed normal findings, except for a delayed H-reflex bilaterally. On day-3 of hospitalization (day-24 of symptom onset) a diagnosis of Guillain-Barré syndrome was considered and intravenous immunoglobulin (IVIg 2 g per kg of body weight) was administered over 5 days. He had aggravation of paresthesias and pains in legs and hands, but there was no ascent of signs. A second NCS was performed on day-29 of symptom onset. The amplitudes of the motor and sensory nerve action potential in the lower limb were slightly decreased. On 34-day of symptom onset (day-5 of completion of the immunoglobulin treatment) one of the family member detected slurred speech (total cumulative dosage of metronidazole at this point: 127.5 g). At this point the patient was transferred to the Neurology wards. Further laboratory tests: thyrotropin, vitamin B12, folate, double-strand DNA, antinuclear antibody, and serum/urine electrophoresis were normal. Neurological examination at this point, finger-to-nose test showed terminal dysmetria. Magnetic resonance imaging (MRI) of brain revealed high-signal lesions in the splenium on diffusion-weighted image (DWI) with a low afferent diffusion coefficient (ADC) map, as well as a high-signal lesion in the bilateral dentate nuclei on fluid-attenuated inversion recovery (FLAIR) images. Eight hours after undergoing brain MRI, the patient complained of dyspnea and excessive diaphoresis and developed blood pressure fluctuation from 100/70 to 180/90 mm Hg (total cumulative dosage of metronidazole at this point: 128.5 g). Electrocardiogram, serum creatinine kinase, lactate dehydrogenase, and troponin T were within normal limits. The next day, metronidazole was stopped. Several hours after discontinuation metronidazole, the autonomic dysregulation settled down. His dysarthria gradually improved over the next 6 days and he also had alleviation of the pains. One week after discontinuing metronidazole, his speech returned to near normal, but the mild ataxic gait remained. Second MRI done one week after the first MRI showed residual hyperintensity in the splenium on FLAIR images and DWI, but not on the ADC map [Figure - 1], B2. Bilateral dentate nuclei lesions nearly disappeared. At 6 months of follow-up, there was partial improvement in the burning sensations. A follow-up NCS was performed at his final visit. Serial MRI and NCS data are shown in [Figure - 1] and [Table - 1]. Discussion The mechanisms of neurotoxicity of metronidazole are unknown. The suggested mechanisms include: inhibition of neuronal protein synthesis, [1] modulation of gamma-amino butyric acid in the cerebellum, [10] or radical injury to nerve tissue. [11] [Table - 2] gives the clinical characteristics of all the published reports of metronidazole neuropathy and encephalopathy. [7],[8],[9],[10],[11],[12],[13] Occurrence of both peripheral neuropathy and encephalopathy in the same individual has been documented. [2],[3],[4],[5],[6],[7],[8] It is likely that occurrence of subclinical neuropathy in association with encephalopathy is much more frequent than reported. The patient reported by Hobson-Webb et al[12] had sensorimotor neuropathy with autonomic neuropathy in the form of vasomotor and temperature dysregulation. However, sequential involvement of peripheral, central, and autonomic nervous systems as in our case involvement as a neurotoxic manifestation of metronidazole has not been documented. From the reported literature it appears that encephalopathy is likely to resolve early and peripheral neuropathy is likely to persist for a long time. [2],[3],[4],[5] Similar were the observations in our patient. Probably this differential pace of resolution of symptoms may be related to the underlying pathology of the neural structure involved. [2] In the brain cerebellar dentate nucleus and midbrain are the most common sites of metronidazole-induced encephalopathy (MIE). [9],[13] Within the brain the resolution of the lesions in different parts of the brain can have different time frames. [4],[5],[9] In our patient the first affection was peripheral nervous system followed by central nervous system and autonomic nervous system. We therefore suggest that a preferential vulnerability of the peripheral nerve may exist among nervous systems, given that toxicity was the first manifestation and the duration of persistent sequelae differed between encephalopathy and autonomic dysregulation. Acknowledgment This work was supported by the 2009 Inje University Research Grant. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11026f1.jpg] [ni11026t2.jpg] [ni11026t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}