 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
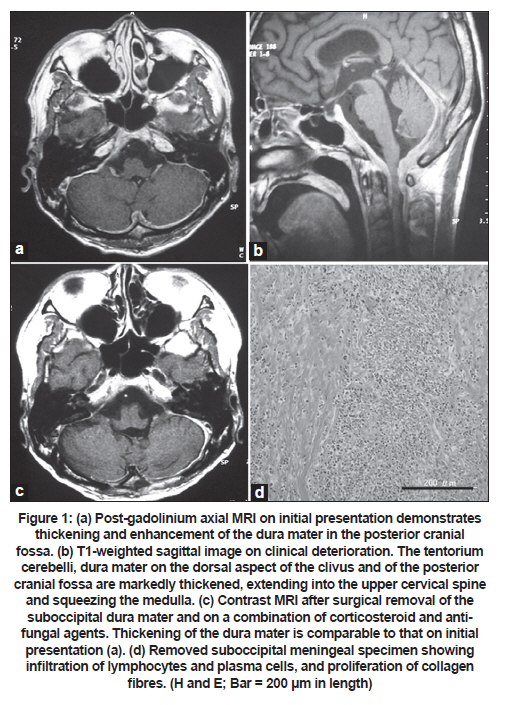
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 111-113 Case Report Hypertrophic pachymeningitis in an immunocompetent adult with positive Aspergillus DNA in the cerebrospinal fluid Hirotaka Kato, Masashi Nakajima, Hiroo Ichikawa, Mitsuru Kawamura Department of Neurology, Showa University School of Medicine, Shinagawa-ku, Tokyo, Japan Keywords: Aspergillosis, central nervous system, corticosteroid, pachymeningitis, polymerase chain reaction Introduction Hypertrophic pachymeningitis is a rare disorder, and the aetiological spectrum includes syphilis, tuberculosis, sarcoidosis, rheumatoid arthritis, Wegener's granulomatosis, multifocal fibrosclerosis, and, in some cases, no cause could be identified. [1] Computed tomography (CT) and magnetic resonance imaging (MRI) showed thickening and enhancement of the pachymeninges. Cerebrospinal fluid (CSF) examination may reveal pleocytosis and erythrocyte sedimentation rate (ESR) may be elevated. The histologic features include fibrotic thickening of the dura mater with cellular infiltrates of lymphocytes, plasma cells, and a few giant cells. Here, we report a patient with hypertrophic pachymeningitis associated with a positive Aspergillus DNA in the CSF. Case Report A 42-year-old previously healthy, HIV-negative man presented with progressive right nuchal pain and headache of two months duration. This was followed by dysphagia and hoarseness. On examination, he was well constituted, fully conscious, and afebrile. His neck was stiff and tender on the right side. Neurological examination revealed right 9 th , 10 th , 11 th , and 12 th cranial nerve palsies. Cranial MRI showed thickening and gadolinium-diethylenetriamine penta-acetic acid (DTPA) enhancement of the tentorium cerebelli and the subtentorial dura mater [Figure - 1]a; MRI of the orbits, sinuses, and nose were unremarkable. ESR was 54 mm at the first hour and C-reactive protein was positive (1.4 mg/dl). Serum VDRL and a purified protein derivative test showed negative results. Rheumatoid factor was mildly elevated (9.0 IU/ml; normal < 7.0) and anti-nuclear antibodies were weakly positive. Levels of serum immunoglobulins were normal. The negative tests included P- and C-antineutrophilic cytoplasmic antibody, angiotensin-converting enzyme, and fungal antigens. CT of the chest and abdomen were unremarkable. CSF examination showed the following findings: opening pressure of 130 mm H 2 O, mononuclear pleocytosis of 43 cells/mm 3 (96% lymphocytes and 4% monocytes), protein content of 100 mg/dl, and glucose level of 56 mg/dl. IgG index was mildly elevated, 1.89 (normal < 1.70). CSF was negative for acid-fast bacillus and Cryptococcus neoformans, Candida albicans, and Aspergillus spp. antigens. (1→3)-β-D-glucan, one of the major structural components of the fungi, was elevated in the CSF (164.0 pg/ml) and normal in the serum (<5.0 pg/dl). [2] A real-time quantitative polymerase chain reaction (PCR) [3] detected 110 copies/ml of Aspergillus-specific DNA in the CSF. With the presumptive diagnosis of hypertrophic pachymeningitis due to Aspergillus infection, the patient was started on oral voriconazole (300 mg daily). The patient showed improvement in his clinical condition in the following weeks. The CSF concentration of (1→3)-β-D-glucan decreased to the normal serum level (<5.0 pg/dl), although no improvement was seen in the CSF and MRI findings. Eight weeks after the introduction of voriconazole, there was rapid deterioration in the patient's condition, with headache, vertigo, nausea and vomiting, dysarthria, and unsteadiness in gait. Neurological examination showed truncal ataxia and gaze-evoked horizontal nystagmus in either direction. Repeat MRI showed compression of the caudal medulla and rostral spinal cord by the thickened pachymeninges [Figure - 1]b. Despite administration of additional oral amphotericin B 400 mg daily, his condition deteriorated further in the level of sensorium. The patient underwent emergency suboccipital craniotomy and decompression of the medulla. The dura mater was opaque, grayish, and rubbery hard, and thickness was 30-40 mm. Microscopic examination showed remarkable proliferation of collagen fibres and infiltration of lymphocytes and plasma cells [Figure - 1]d. There were no necrotic foci, granulomas, or necrotising vasculitis. Extensive search with Grocott stain failed to show fungal hyphae. Intravenous dexamethasone 0.4 mg/kg/day, intravenous liposomal amphotericin B 1.0 mg/kg/day, and oral flucytosine 500 mg/kg/day were started immediately after surgery. At repeat MRI -four weeks after surgery, the dura was seen less thick, but still enhancing [Figure - 1]c. Intravenous amphotericin B for two weeks was replaced by oral fluconazole for eight weeks. Dexamethasone dose was tapered and discontinued in 12 weeks. Currently, 30 months after completion of treatment, the patient is independent despite the presence of mild dysphagia and dysarthria. Discussion The patient in our study had progressive hypertrophic pachymeningitis, with the tentorium cerebelli and posterior cranial fossa extending to the cranio-cervical junction. The CSF analysis showed pleocytosis, which is suggestive of an inflammatory process. However, an extensive laboratory workup for microorganisms or autoimmune disease failed to find a definite aetiology, except for the presence of (1→3)-β-D-glucan and Aspergillus DNA in the CSF. (1→3)-β-D-glucan is one of the major structural components of fungi. The release of soluble (1→3)-β-D-glucan into the culture fluids by C. albicans and A. fumigatus parallels with the growth of the fungi. [2] Although the CSF assay of (1→3)-β-D-glucan is not established, in this patient, the concentration was high in the CSF but normal in the serum; moreover, the CSF concentration decreased with voriconazole therapy. High sensitivity of PCR assay in the detection of Aspergillus spp. in the CSF has been demonstrated in patients with cerebral aspergillosis. [4],[5] Real-time PCR assay allowed quantification of pathogen DNA as well as detection of most of the clinically relevant Aspergillus spp. [3] We presume that, in this patient, Aspergillus spp. was present in the CNS at the initial presentation, and antifungal voriconazole may have limited proliferation of the fungus. Our patient had progressive pachymeningeal hypertrophy and histology showed that extensive fibrosis and infiltration of lymphocytes and plasma cells. Aspergillosis is rare in people with intact immunity and host defenses, although occasional cases of isolated CNS infection are recorded. [6] The histological findings of CNS aspergillosis depend on the underlying immune status of the patient. Granulomatous inflammation with giant cells and fibrosis is seen in more chronic lesions, when cell-mediated immunity is preserved and fungal load is less. [7] After dexamethasone, in combination with antifungal agents, thickness of the dura mater regressed and the patient's clinical condition improved and stabilised. In order to facilitate the diagnosis of cerebral aspergillosis, non-culture-based methods have been developed in recent years. [2],[3],[4],[5] We hypothesised that, in this patient, intact immune status and less burden of Aspergillus infection may have resulted in a chronic progressive hypertrophic pachymeningitis. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11028f1.jpg] |
| |||||||||

{kind=link}