 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
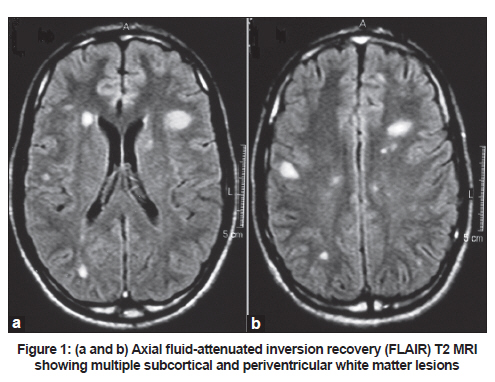
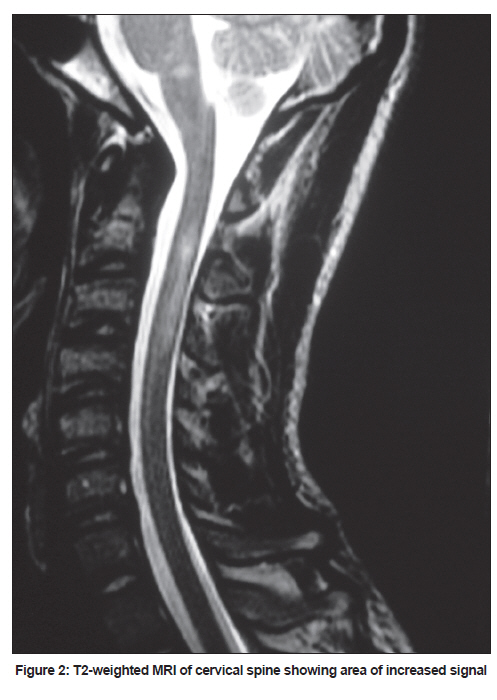
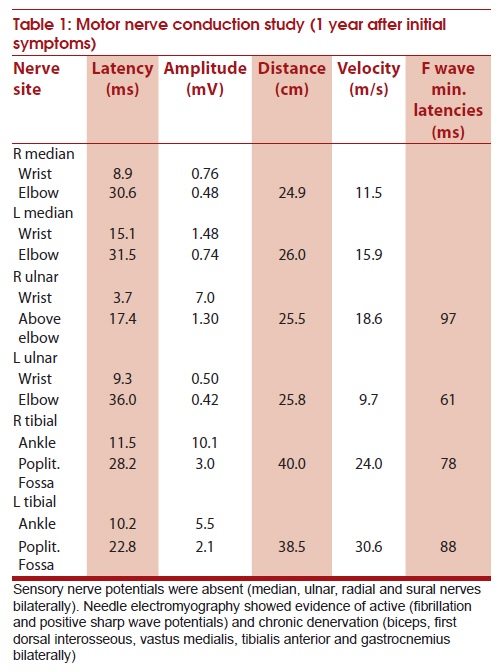
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 114-116 Case Report Hepatitis C virus: A rare manifestation - Remitting relapsing central and peripheral demyelination Marcio Luiz Escorcio Bezerra1, Juliana Arita Harumi1, Jullyanna Sabrysna Morais Shinosaki1, José Luiz Pedroso1, Camila Catherine Henriques de Aquino1, Larissa Teles de Souza1, Robson Fantinato Baiense1, Acary Souza Bulle de Oliveira2 1 Department of Neurology, Federal University of São Paulo, São Paulo SP, Brazil Keywords: Central and peripheral demyelination, hepatitis C virus infection, negative cryoglobulins, vasculitis Introduction The common neurologic manifestations of hepatitis C virus (HCV) include axonal type of peripheral neuropathy and encephalopathy. The neurological complications of HCV are mostly related to mixed cryoglobulinemia, and vasculitis is the main pathogenic mechanism. [1],[2],[3],[4] Neurologic involvement with no cryoglobulinemia in HCV is rare and only a fewer reports of demyelinating lesions have been documented, [1],[2],[3] In this report we present a patient with HCV and remitting and relapsing central and peripheral demyelination. Case Report A 17-year-old previously healthy male was admitted for pain and ascending weakness of left lower limb of six weeks duration. In the next week he developed similar complaints in the right lower limb, weakness of both the upper limbs and difficulty to walk. Within the next three weeks, he developed dysphagia and left ptosis. Neurologic evaluation at this admission revealed dysphonia and dysarthria, left partial ptosis, left sixth cranial nerve palsy, bilateral palatal palsy, and quadricparesis with distal predominance. Deep tendon reflexes were absent in the lower limbs and diminished in the upper limbs and bilateral plantars were unequivocal. Sensory examination showed hypoalgesia in the distal third of the four limbs and absent vibratory sensation in hands and feet. Liver enzymes aspartate transaminase (AST; 232 IU/L) and alanine transaminase (ALT; 392 IU/L), were initially elevated and settled few days later. Routine blood biochemistry including Remaining thyroid functions, serum protein electrophoresis, vitamin B12 and folate levels were normal. Screening tests for antinuclear antibody, rheumatoid factor, anti-neurtrophilic cytoplasmic antibodies (ANCA), cryoglobulins, C3, C4 and anti-aquaporin-4 were negative. Microbiological screening for infection (serum) was indeterminate for HCV and negative for the remaining, including human immunodeficiency virus (HIV), hepatitis B, cytomegalovirus (serum), herpes simplex virus, herpes zoster virus, Treponema pallidum and Mycobacterium tuberculosis (serum and spinal fluid). Cerebrospinal fluid analysis showed 594 mg/dL proteins and 55 cells/mL (predominantly lymphocytes). Brain and spinal cord magnetic resonance imaging (MRI) scan revealed multiple subcortical and periventricular white matter lesions, hyperintense in T2-weighted images and hypointense in T1, some of them enhanced with gadolinium (Gd) enhancement [Figure - 1]. Cervical spinal cord showed non-enhancing intramedullary signal changes similar to the cerebral lesions [Figure - 2]. Electromyographic study showed demyelinating polyneuropathy which at this admission was considered to be acute. He received 5-day treatment of intravenous immunoglobulin (IVIg, 0.4 g/kg/day) and was also initiated on prednisone (1 mg/kg/day). He showed immediate improvement in the muscle power and other neurologic deficits which was marked over the next few months. During the follow-up, previously indeterminate HCV serology as well as polymerase chain reaction (PCR) for HCV virus were positive. After six months after the first admission patient presented with clinical features of myelopathy: pyramidal quadriparesis and bladder dysfunction. Repeat CSF examination showed slight increase in cells (23 cells/mL, predominantly lymphocytes) and protein (78 mg/dL) levels. Repeat cervical MRI scan showed contrast enhancing new lesions, predominantly in cervicothoracic segment. Brain MRI showed an improvement of previous cerebral lesions. He was give corticosteroid pulse treatment and was put on oral prednisone 20 mg/day. He showed a gradual recovery. Liver biopsy showed active inflammation and he was put on alpha interferon and corticosteroids for HCV. As he had worsening of neurological deficits after one month of antiviral treatment, interferon was stopped. He remained asymptomatic for about an year, when he developed areflexic motor weakness and wasting of all the four limbs. Repeat CSF analysis showed 139 mg/dL proteins and 15 cells/mL (predominantly lymphocytes). Repeat cranial and spinal MRI demonstrated significant improvement in the earlier lesions and no new lesions. Electrodiagnostic study showed predominantly demyelinating neuropathy [Table - 1] and the diagnosis of chronic inflammatory demyelinating polyradiculoneuropathy was considered. Patient was given another course of IV Ig. He showed gradual improvement and on maintenance dose of oral prednisone. Discussion In our patient HCV infection was complicated by remitting and relapsing central and peripheral demyelination. Mostly peripheral neuropathy in patients with HCV infection is axonal type of symmetrical sensorimotor neuropathy or mutifocal mononeuropathy. The underlying pathogenetic mechanisms for this complication are vasculitis and systemic cryoglobulinemia. [1],[2],[3],[4],[5] Peripheral demyelinating neuropathy has been rarely described, most often in cryoglobulin negative patients. [6],[7],[8],[9] In central nervous system, vasculitis is a major pathogenic mechanism, associated cryoglobulinemia. [1],[2] Few reports of inflammatory syndromes involving central nervous system, encephalomyelitis have been reported in patients with HCV with no cryoglobulinemia or vasculitis. [10],[11] Our patient had chronic demyelinating neuropathy [12] and MRI evidence of white matter lesions. In the absence of vasculitis and cyroglobinemia the MRI cerebral white matter lesions and cervical spinal cord lesions have been interpreted as demyelinating plaques. There has been report of one patient with central and peripheral demyelination, however, in this patient the onset of the demyelinating process was not simultaneous. [4] Our patient had clinical worsening with interferon alpha and this complication has been well documented in the literature. [13],[14] Sensory nerve potentials were absent (median, ulnar, radial and sural nerves bilaterally). Needle electromyography showed evidence of active (fibrillation and positive sharp wave potentials) and chronic denervation (biceps, first dorsal interosseous, vastus medialis, tibialis anterior and gastrocnemius bilaterally) References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11029f1.jpg] [ni11029f2.jpg] [ni11029t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}