 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
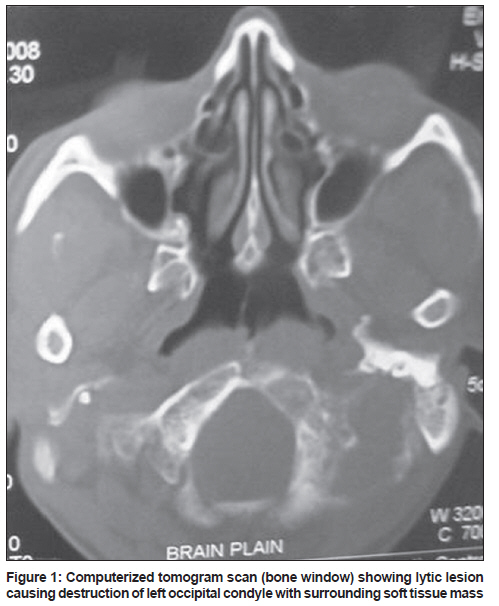
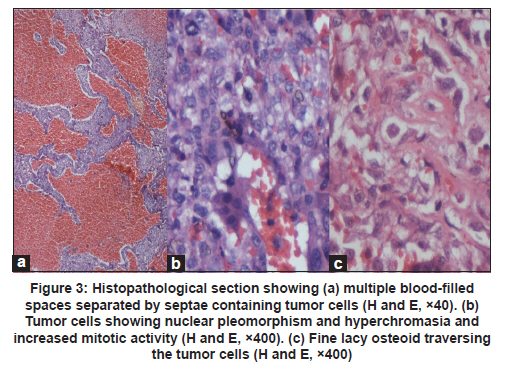
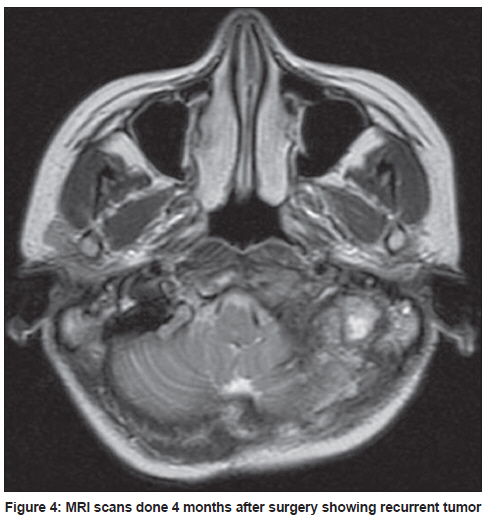
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 117-119 Case Report Primary telangiectatic osteosarcoma of occipital bone: A case report and review of literature Mohana Rao Patibandla1, Shantveer G Uppin2, Amit Kumar Thotakura3, Manas K Panigrahi4, Sundaram Challa2 1 Department of Neurosurgery, Nizam's Institute of Medical Sciences, Hyderabad, India Date of Submission: 23-Jun-2010 Code Number: ni11030 Abstract Telangiectatic osteosarcoma (TOS), an uncommon variant of osteosarcoma, involving skull bones is extremely rare. We present clinico-pathological, imageological and treatment outcome of a primary TOS of occipital bone in a 30-year-old woman and review the previously reported skull bone TOS. We suggest that TOS should be included in the differential diagnosis of destructive lytic lesions involving the skull bones. As radical surgical procedures are not applicable to skull bones, the outcome is poor even with adjuvant chemotherapy.Keywords: Lytic lesion, occipital bone, osteosarcoma, posterior fossa, telangiectatic Introduction Extragnathic osteosarcoma involving skull bones is uncommon. Telangiectatic osteosarcoma (TOS), an uncommon variant of osteosarcoma, involving skull bones has been rarely reported and to date, only 5 cases of TOS involving the skull bone have been reported in the world literature. [1],[2],[3],[4] Case Report A 30-year-old woman was brought to the Emergency Department with a 15-day history of occipital headache and 2-day history of nausea and two episodes of vomiting. Clinical examination revealed fine nystagmus and bilateral papilledema. Computerized tomogram (CT) scan of skull (bone window) showed a lytic lesion causing destruction of left occipital condyle with surrounding soft tissue mass with extension into the posterior fossa up to petrous bone [Figure - 1]. On magnetic resonance imaging (MRI), it was a well-defined, extra-axial mass measuring 4 × 3 × 3.5 cm, involving the left occipital condyle with extension into posterior fossa causing mass effect on fourth ventricle. The mass was hyperintense on T2WI and predominantly hypointense on T1WI with heterogenous enhancement after administration of contrast [Figure - 2]a and b. Near-total excision of the tumor was done by left far lateral approach with placement of left frontal reservoir. Peroperatively, the tumor was found to be reddish, hemorrhagic, highly vascular and non-suckable. It was well demarcated from cerebellum and showed areas of necrosis and calcification. The tumor was seen eroding occipital bone with extension up to lateral border of C2 vertebra and infiltration into sub-occipital muscles. The patient had an uneventful postoperative period and was discharged on seventh postoperative day. Histopathological examination revealed multiple blood-filled spaces of variable sizes lined by spindle cells and giant cells [Figure - 3]a. The intervening area showed spindly-to-polygonal tumor cells with oval-to-elongated pleomorphic, hyperchromatic nuclei. Mitotic figures were frequent, including the atypical mitotic figures [Figure - 3]b. Admixed with these cells, there were tumor giant cells and osteoclastic giant cells. Focal areas showed thin lacy osteoid traversing the tumor cells [Figure - 3]c. Immunohistochemistry with CD 31 was negative in tumor cells, ruling out the possibility of angiosarcoma. The above histological features were consistent with the diagnosis of TOS. Bone scan; and CT scan of chest, abdomen and pelvis showed no evidence of systemic involvement. Postoperative CT scans done 2 weeks after surgery showed contrast enhancement at the surgical margins, suggestive of residual tumor. Postoperatively the patient received 53 Gy of radiation over 6 weeks in 30 fractions, followed by 6 cycles of cisplatin, adriamycin and ifosphamide-based chemotherapy. Follow-up CT and MRI scans at 4, 6, 9 and 12 months showed recurrence of tumor with progressively increasing size [Figure - 4]. The patient succumbed to the disease at 16 months after surgery in spite of aggressive adjuvant radiotherapy and chemotherapy. Discussion Osteosarcoma (OS) is the most common primary malignant bone tumor presenting in childhood and adolescence. The head and neck osteosarcomas account for 0.5% to 8.5% and 75% to 88% with location in jaws. [5] TOS accounts for 0.4% to 12% of all skeletal osteosarcomas. [2],[6] These tumors commonly (75%) occur in the metaphyseal region of long bones [7] , but are known to arise from mandible, vertebrae, scapula and innominate bone. [7] Extragnathic TOSs have been rarely reported at unusual sites such as sphenoid bone [4] and frontal bone. [3] The hallmark of TOS is expansile lytic lesion without sclerosis [6] and often exhibits heterogenous high signal intensity on T2WI and fast spin T2WI and may also show zones of high signal intensity on T1WI and proton density (PDWI) corresponding to areas of hemorrhage. These tumors show prominent gadolinium enhancement. [4],[7] Fluid-fluid level is a nonspecific feature, which represents the hemorrhage. [8] Radiologically the closest possible differential diagnosis for TOS is aneurysmal bone cyst, giant cell tumor or angiosarcoma and histopathology examination is essential to diagnose these tumors. [4],[8] TOS should be considered as a diagnostic possibility when either CT or MR studies show a lytic lesion with fluid-fluid levels. [4],[6],[8] However, our patient did not show the fluid-fluid levels. All cases of skull bone TOS, so far reported including our case, have shown characteristic radiological features. [3],[4] Histopathological studies in correlation with imageological findings are essential for the diagnosis of TOS. [8] The histological and radiological diagnostic criteria proposed by the World Health Organization include: 1) predominantly lytic bone mass with minimal sclerosis; 2) grossly cystic medullary mass with no or minimal solid or sclerotic component; and 3) histologic features consisting of bone-forming tumor with notable blood-filled spaces separated by septae lined by, and/ or containing, malignant tumor cells with prominent nuclear atypia and limited osteoid deposition. [9] Histological findings of all the previously reported cases of skull bone TOS, including the present case, were characteristic. [1],[2],[3],[4] Treatment modality of TOS involves a combination of aggressive surgery with good margins, radiotherapy and multi-agent chemotherapy. [4] Though TOS is highly chemo-sensitive compared to conventional OS, [10] at present, using multi-modality therapy, the outcomes of TOS and conventional type are considered similar. [2],[8] Neoadjuvant chemotherapy can be administered to these patients if diagnosis can be achieved before surgery on a biopsy, which is not possible in all skull base tumors. Local recurrence is the major cause of death in skull bone osteosarcomas. The two important factors that are predictive of better outcome are (i) absence of local progression on chemotherapy and (ii) use of three or more chemotherapeutic agents. [8] References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11030f4.jpg] [ni11030f3.jpg] [ni11030f1.jpg] [ni11030f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}