 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
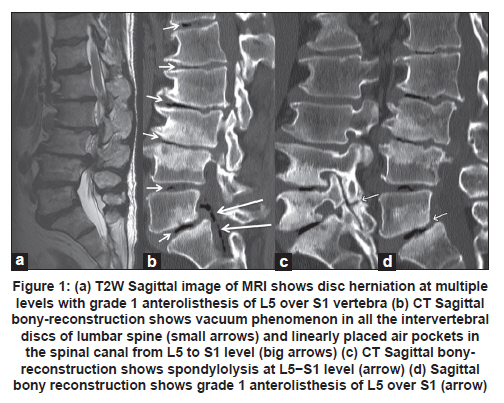
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 120-121 Case Report A rare association of spontaneous pneumorrhachis with spondylolisthesis and lumbosacral vacuum phenomenon: A case report with review of literature Sunitha P Kumaran, Kanchan Gupta, Shambanduram Somorendra Singh Department of Radiology, Sri Sathya Sai Institute of Higher Medical Sciences, Bangalore, India Spontaneous pneumorrhachis, non-traumatic, non-iatrogenic air within the spinal canal, is a very rare occurrence. We report a case of spontaneous pneumorrhachis, multiple air pockets in the epidural space, with vacuum discs and spndylolisthesis. Probably this is the first report of such case. Keywords: Spondylolisthesis, spondylolysis, spontaneous pneumorrhachis Introduction Spontaneous pneumorrhachis is very rare. Most cases of pneumorrhachis are secondary to medical procedures, trauma, pneumothorax, or pneumomediastinum. [1] We report a patient with air in the spinal canal and intradiscal spaces associated with grade 1 spondylolisthesis and discuss the probable mechanisms of spontaneous pneumorrhachis. Case Report A 51-year-old man presented with history of chronic low back pain. No past history of surgery or trauma was present. Neurologic examination was essentially normal. Magnetic resonance imaging (MRI) of the spine showed grade 1 anterolisthesis of L5 over S1 vertebra, disc herniation at multiple levels [Figure - 1]a. For bony details, computerized tomography (CT) was done, which showed vacuum phenomenon in all the lumbar intervertebral discs [Figure - 1]b. Linearly placed air pockets were noted within the spinal canal anterior to the thecal sac from L5 to S1 levels [Figure - 1]b. A diagnosis of pneumorrhachis was made. There was also grade 1 anterolisthesis of L5 over S1 [Figure - 1]c with spondylolysis [Figure - 1]d. The patient was planned for surgery for the correction of spondylolisthesis which was the cause of back pain. Discussion Free air in the spinal canal is a rare occurrence and was first reported by Gordon et al. in 1977 [2] and Newbold et al. [3] introduced the term pneumorrhachis in 1987. There were documentation of very few cases since then. The etiologic factors include spontaneous pneumomediastinum, traumatic pneumothorax, skull fracture, epidural anesthesia, radiation therapy, and thoracic surgery. [4] Spontaneous pneumorrhachis denotes non-traumatic, non-iatrogenic air within the spinal canal and is a very rare occurrence. Different pathways of air entry into the spinal canal are postulated. According to Coulier, [5] the pathogenesis of pneumorrhachis is due to "valve pump mechanism" or "ball valve effect", wherein the gas collected in the clefts of a long-standing diseased disc is expulsed through a weak spot or rent in the annulus fibrosus as a sequelae to disc degeneration. The radiological findings of vacuum phenomenon with degenerative discs were described by Knutsson [6] in 1942. Marr [7] in 1955, found gas in the intervertebral disc in 2.036% of his cases, whereas Gershon-Cohen et al.[8] found the vacuum phenomena in 20.8% of their cases. According to Gulati et al.,[9] the vacuum phenomenon is due to creation of space in a degenerative intervertebral or apophyseal joint due to motion, especially extension. The expanded space thus created is filled with gas evolved from the surrounding extracellular fluid. Gas in the intervertebral joint space was analyzed by Ford and colleagues [10] and was found to contain 90−95% nitrogen. According to Kim, [11] intradiscal gas accumulation and repeated microtrauma causing erosive defects in the endplates/detachment of annulus lead to pneumorrhachis. Similarly in our case, all the extra discal air must have migrated from the intradiscal vacuum adjacent to endplate. In addition spondylolisthesis might have contributed to the migration of air into the spinal canal. Most of the time it is asymptomatic. Kyung-Jin Song et al.[12] reported a case of spontaneous extradural pneumorrhachis causing cervical myelopathy. CT spine is the imaging modality of choice. [13] Most authors recommend conservative treatment for the intraspinal gas. [11] Bosser et al.[13] reported CT-guided aspiration of pneumorrhachis but in his case, epidural gas recurred and was subsequently removed by surgical treatment. The aspiration was considered incomplete treatment, since the origin of the air still remained. If there is causative neurological deficit or frequent recurrence, surgical decompression using the lateral transmuscular approach can be done. [14] Pneumorrhachis usually represents an asymptomatic epiphenomenon but can also be symptomatic by itself as well as by its underlying pathological causes. The diagnostic procedure should include spinal CT, which is the imaging modality of choice. It should be differentiated from free intraspinal gas collections, which can be due to degenerative, malignant, inflammatory and infectious diseases by gas-forming organisms. A multidisciplinary approach is required for the management, which is mainly directed to the associated pathologies to enable adequate therapy. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11031f1.jpg] |
| |||||||||

{kind=link}