 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
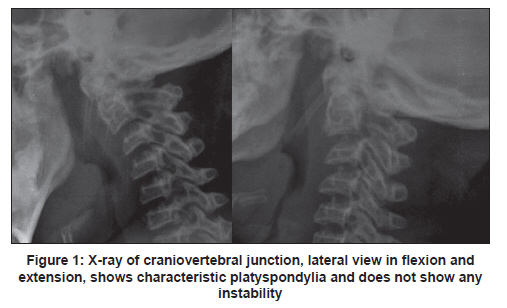
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 126-127 Letter to Editor Myelopathy in a dwarf: A case of Morquio's syndrome without odontoid hypoplasia Dhaval Shukla, S Arvind, B Indira Devi Department of Neurosurgery, NIMHANS, Bangalore, India Morquio's syndrome is a type IV mucopolysaccharidoses (MPS) characterized by deposition of mucopolysaccharides in connective tissue and cartilage ground substance with excretion of keratan sulfate in urine. The characteristics of this disease are dwarfism with normal intelligence and various skeletal dysplasias. Involvement of craniovertebral junction can result in cervical myelopathy. [1] A 20-year-old lady, a known case of Morquio's syndrome developed insidious-onset, gradually progressive weakness and stiffness of lower limbs after a fall (3 months). On examination: single breath count of 12; weight 21 kg; height, 112 cm (< 10 th centile); arm span, 101 cm; and head circumference, 52 cm. There was bilateral corneal clouding, restricted mouth opening, short and restricted neck, and receding chin. The limbs were short with stiff joints and fixed flexion deformity of shoulder, elbow, wrist and knee. The fingers were short and stubby with thumb in the same plane as fingers. The phenotype was suggestive of Morquio's syndrome. Neurological examination revealed normal intelligence, visual acuity of 6/26 in right eye and 6/60 in left eye with normal visual fields and ocular fundi. She had hypertonia in lower limbs, and muscle power was 5/5 in upper limbs and 4/5 in lower limbs. Except for impaired joint and position sensations in all the four limbs, sensory examination was unremarkable. The plantar response was extensor on both sides, and deep tendon jerks were exaggerated in all the four limbs. The gait was spastic. Routine blood parameters were normal. Pulmonary function tests revealed severe restrictive abnormality. Ultrasound of abdomen showed a mild hydronephrosis on the right. Ovaries were absent and uterus was small. Echocardiography showed signs of rheumatic heart disease. X-rays of the spine showed the characteristic universal platyspondyly and fused C2 and C3 spinous processes. Flexion and extension studies of craniovertebral junction did not show atlanto-axial instability [Figure - 1]. Computer tomography (CT) scan of craniovertebral junction showed a sclerosed and well-developed odontoid process. The atlanto-odontoid distance was normal. Magnetic resonance imaging (MRI) of craniovertebral junction showed soft tissue mass compressing the spinomedullary junction at level of foramen magnum to C2 vertebra [Figure - 2]. She underwent posterior approach; foramen magnum decompression, C1 and C2 posterior arch excision and removal of thick connective tissue compressing the dura. No fixation procedure was done. She improved significantly during the postoperative period; and at follow-up after 10 months, she was asymptomatic. Postoperative X-ray of craniovertebral junction did not reveal atlanto-axial instability. Our patient had phenotype suggestive of Morquio's syndrome, which was already diagnosed during her childhood and hence we did not confirm with urinary keratan sulfate test. On imaging, the characteristic spinal deformity in Morquio's syndrome is platyspondylia (flat vertebra). [2] The other X-ray findings of Morquio's syndrome are, hypoplastic or absent dens with C1/C2 instability, anterior tongue of thoracic vertebrae, hook-shaped lumbar vertebral bodies, and wide disc spaces. [3] MRI findings are spinal cord compression at C1/C2. [2] Patients with this syndrome present to neurosurgeon with chronic compressive high cervical myelopathy with involvement of corticospinal tract, posterior columns and spinothalamic tract in descending order. The pathogenesis of myelopathy is atlanto-axial subluxation, stenosis of foramen magnum or atlas and compression by soft tissue mass both anteriorly as well as posteriorly. [4],[5] Treatment depends on site of compression and presence of instability. The peculiarity of this case was absence of hypoplastic odontoid process and instability. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11033f2.jpg] [ni11033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}