 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
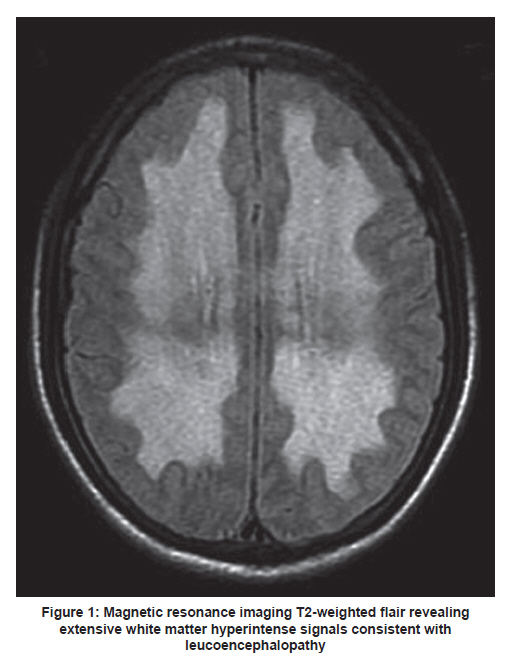
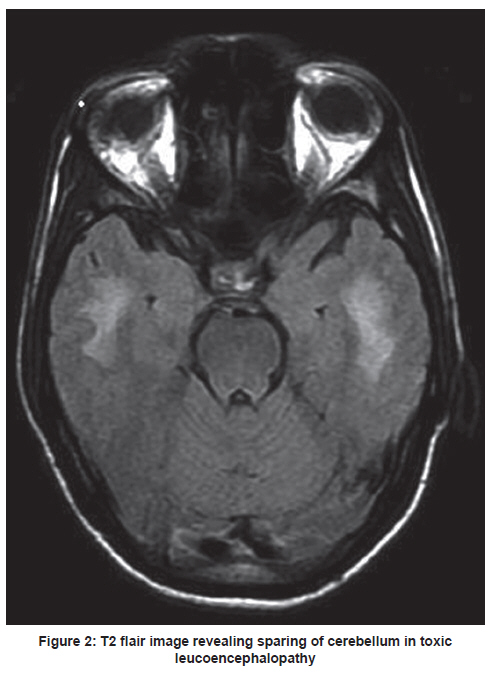
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 127-128 Letter to Editor A rare case of acute fatal leucoencephalopathy due to heroin exposure Rajesh Verma, Pawan Sharma, Mukund R Vidhate Department of Neurology, Chhatrapati Sahuji Maharaj Medical University, Lucknow, Uttar Pradesh, India Toxic spongiform leucoencephalopathy caused by inhalation of heroin vapor is one of the causes of acquired toxic leucoencephalopathy. [1] We report a patient with acute leucoencephalopathy due to heroin exposure with unusual magnetic resonance imaging findings. A previously healthy 25-year-old young man, inhaling smack for the past 4 months, presented with acute onset fever and altered sensorium of 10 days duration. On examination, he was in altered sensorium. There was spasticity of all the four limbs with hyper-reflexia and extensor planter response. Plain and contrast CT head showed bilateral symmetrical hypodensities of white matter in periventricular and centrum semiovale regions. The lesions were hypointense on T1-weighted, hyperintense on T2-weighted, and fluid attenuated inversion recovery (FLAIR) magnetic resonance imaging (MRI) sequences [Figure - 1]. The lesions were bright on diffusion weighted imaging (DWI) with low apparent diffusion coefficient (ADC) showing restriction of diffusion. The routine laboratory examination including cerebrospinal fluid (CSF) studies were normal. Other investigations including serological test for HIV, herpes simplex virus, and JC virus were negative. The final diagnosis of toxic leucoencephalopathy due to smack inhalation was based on patient's history, neurological examination, and characteristic neuroimaging findings. Progressively, patient became unresponsive and succumbed to illness after 5 days. Spongiform leucoencephalopathy is a distinct entity caused by heroin inhalation, first reported by Wolters et al. in 1982, in addition to other neurological complications such as cerebral infarction, cerebral hemorrhage. [2] Heroin-induced spongiform leucoencephalopathy is more common after inhaling heated heroin vapors, although rarely reported after intravenous abuse. It may be related to aluminium foil used for inhalation or to the impurities and adulterants added to heroin. [3] Most of the patients present with acute or subacute onset cerebellar ataxia, dysarthria, akinetic mutism, and spastic quadriparesis. [4] In some patients, this can be rapidly progressive culminating in death. [5] The histopathological hallmark of spongiform leucoencephalopathy is vacuolar degeneration of cerebral white matter tracts. Electron microscopy shows fluid entrapment between the myelin lamellae and absence of demyelination in these patients. [6] MRI most commonly shows bilateral symmetrical hyperintense lesions in the white matter of the cerebrum and cerebellum on T2-weighted images. In our patient, MRI revealed extensive symmetric involvement of white matter of the cerebral hemispheres and total sparing of the infratentorial compartment [Figure - 2]. Blasel et al. described rare MRI findings in three patients where infratentorial structures were not involved. [7] The acute presentation mimicking acute meningoencephalitis and sparing of cerebellum, internal capsule, and brainstem on MRI are unusual features in our patient. In addition, the finding of restricted diffusion on DWI/ADC suggests the possible role of hypoxia in acute fatal toxic leucoencephalopathy. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11034f2.jpg] [ni11034f1.jpg] |
| |||||||||

{kind=link}
{kind=link}