 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
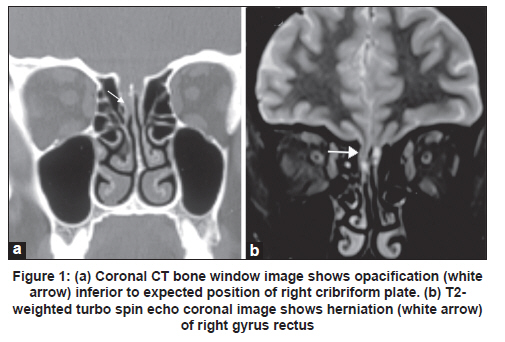
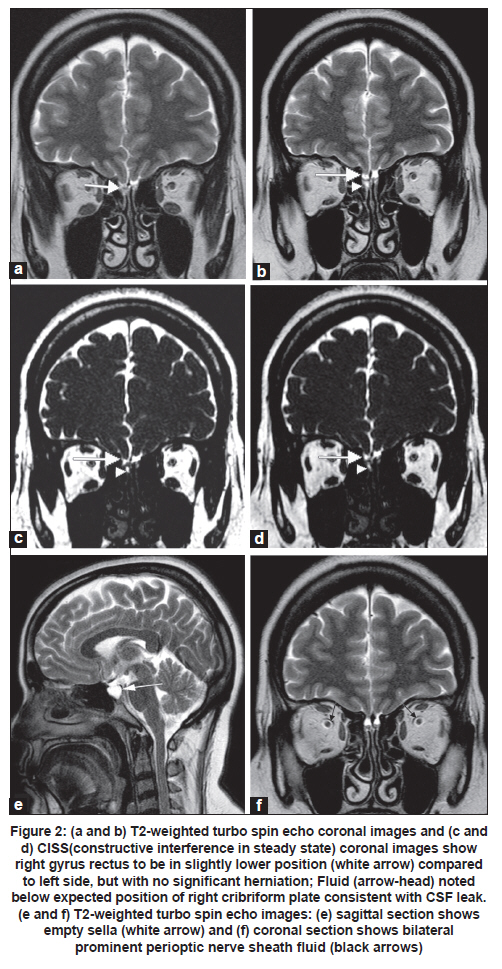
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 131-132 Letter to Editor Intermittent herniation of brain: A rare cause of intermittent cerebrospinal fluid rhinorrhea Anitha Sen, Chandrasekharan Kesavadas Imaging Sciences & Interventional Radiology, SCTIMST, Thiruvananthapuram, Kerala, India We report a case of a 48-year-old female who presented with complaints of intermittent episodes of watery discharge from right nostril since 4-5 months, which increased on bending forward and on straining. There was no history of headache, vomiting, visual symptom or head injury. Neurological and ophthalmological examinations were normal. Plain CT through the anterior cranial fossa showed opacification inferior to expected position of right cribriform plate [Figure - 1]a. No leak could be demonstrated in the CT cisternography. MRI done after 2 weeks during an asymptomatic (no rhinorrhea) period revealed herniation of right gyrus rectus [Figure - 1]b. Repeat MRI performed at the time of active cerebrospinal fluid (CSF) leak showed the right gyrus rectus to be in a slightly lower position compared to left side, but there was no significant herniation of brain [Figure - 2]a. Fluid appeared to extend below the cribriform plate level on right side [Figure - 2]b, c and d. Empty sella [Figure - 2]e and bilateral mildly prominent perioptic nerve sheath fluid [Figure - 2]f was also noted. We presume that herniation of brain had sealed the site of leak at the time of first MRI, leading to stoppage of leak. Later, in the second MRI done when the rhinorrhea recurred, the site was not plugged with herniated brain. Patient had a temporary cessation of CSF rhinorrhea lasting for a few weeks following lumbar puncture on two occasions: first time after the CT cisternography and second time after lumbar puncture done for ruling out meningitis. Decrease in CSF pressure after LP may have caused sagging of brain and herniation of gyrus rectus, leading to plugging of osteodural defect and cessation of CSF rhinorrhea. To the best of our knowledge, intermittent cerebral herniation leading to intermittent CSF rhinorrhea has not been reported previously. There have been case reports regarding intracranial hypertension as etiology of CSF rhinorrhea [1],[2] and encephalocele. [2] But in our case, other than empty sella and mildly prominent perioptic nerve sheath fluid, other classical radiological signs of intracranial hypertension such as vertical buckling of optic nerve and flattening of the posterior sclera were absent. Empty sella has a 60% incidence [3] in spontaneous CSF rhinorrhea and 76% incidence in females with spontaneous CSF rhinorrhea. In our patient there was no clinical suspicion of intracranial hypertension or evidence of papilloedema. Since the rate of CSF fistula detection is significantly low in patients without active leak compared to patients with active leak, [4] many institutions by protocol, image CSF leaks only during periods of active leak. Our case indicates that imaging during asymptomatic period also may have some value and may throw light on the cause of 'intermittency' of CSF leaks. In particular, role of intracranial pressure in the etiology and intermittency of CSF leaks needs to be studied. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11037f2.jpg] [ni11037f1.jpg] |
| |||||||||


{kind=link}
{kind=link}