 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
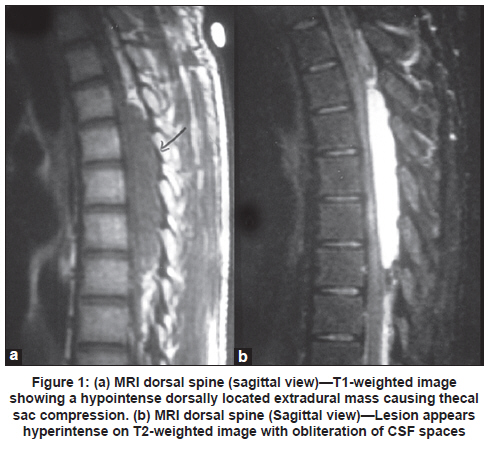
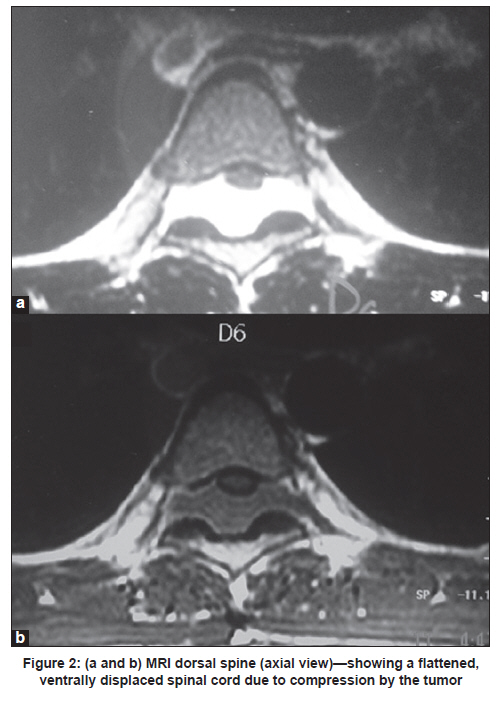
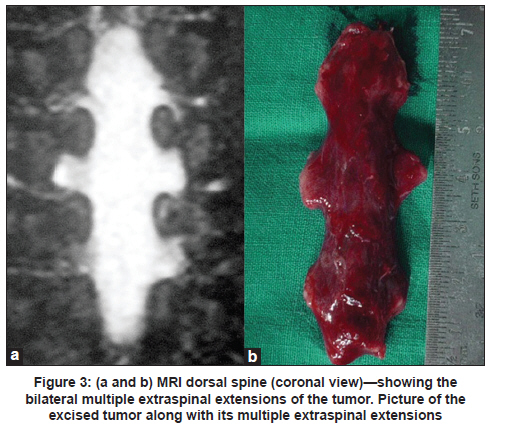
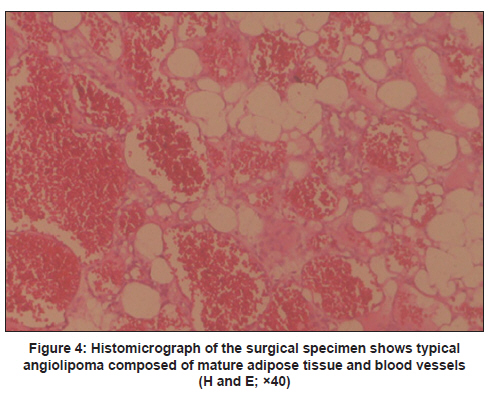
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 134-136 Letter to Editor Thoracic epidural angiolipoma with bilateral multilevel extraspinal extensions: A rare entity Batuk Diyora, Naren Nayak, Sanjay Kukreja, Hanmant Kamble, Alok Sharma Department of Neurosurgery, L.T.M.G. Hospital, Mumbai, India Spinal angiolipomas are rare benign tumors and account for 0.04-1.2% of all spinal tumors and 2-3% of spinal extradural tumors. [1],[2],[3],[4] We present the operative findings and MRI features of a noninfiltrative angiolipoma with bilateral multilevel extraspinal extensions. A 20-year-old male presented with upper abdominal pain, radiating to back, for the past 6 months and bilateral lower limb weakness since 1 week. Neurological examination revealed paraparesis and impaired sensation below T4 level. Deep tendon reflexes were hyperactive and plantar response was bilateral extensor. Magnetic resonance imaging (MRI) of the spine [Figure - 1]a and b showed a space occupying lesion from T5 to T8 vertebral levels located in the posterior epidural space. It was spindle shaped, measuring 6.5 cm in length and 12 mm at maximum width and extending bilaterally into the extraspinal space through neural foramina. It was isointense on T1-weighted images and hyperintense on T2-weighted images [Figure - 2]a and b and showed enhancement with contrast. The patient underwent T4-T9 laminectomy with total removal of epidural mass. Intraoperatively, the mass was reddish, soft to firm, fleshy with minimal vascularity. It had bilateral, multilevel, extraspinal extensions with widening of the neural foramina. There was a good plane of cleavage between the mass and dura. Extraspinal extensions of the mass were dissected through the widened foramina on either side [Figure - 3]a and b. A satisfactory decompression of the spinal cord as well as nerve roots was achieved. Histopathology revealed angiolipoma [Figure - 4]. Patient had a complete neurological recovery over the next 3 months. Angiolipoma is a subgroup of lipoma, also known as hemangiolipoma, angiomyolipoma, and fibromyolipoma. [5] The pathogenesis of spinal angiolipoma is unknown. Their probable origin is from progenitor tissue as lipoma and hemangioma. [4] Their preponderance in peri- or postmenopausal women supports a role of hormonal influence. Pathologically, the lesion is composed of mature fat cells and capillaries with some fibrin thrombi. Presence of fibrinous microthrombi in the lumen is a diagnostic feature. Degenerative changes (i.e., hyalinization, myxoid change, and fibrosis) may be present in longstanding cases. Angiolipomas are of two types: noninfiltrating and infiltrating. [6] Noninfiltrating angiolipomas are more common. They are encapsulated lesions which present with painful, soft subcutaneous nodules. Infiltrating angiolipomas are rare, usually involve the extremities and may extensively infiltrate into the surrounding tissues. Progressive paraparesis, back pain without radiculopathy, lower extremity sensory changes, and hyperreflexia are the usual clinical presentations. Unusually, patient can present with sudden-onset paraparesis. Exacerbation of symptoms may occur during pregnancy and in obese patients probably because of hormonal changes and increase in fatty component within the angiolipoma. [5] However, the association of spinal angiolipoma with increased body mass index has not been systematically studied. [7] MRI reveals a solid mass that is usually hyperintense on T1 than T2-weighted signals, but can also be of heterogeneous or mixed intensity. It may be isointense with fat suppression sequences. Because of the presence of capillaries and venous channels, angiolipoma does not contain vascular flow void on MRI. Complete surgical excision of the lesion is the treatment of choice. Complete excision is always possible in noninfiltrating angiolipoma and difficult in infiltrating angiolipomas, especially when it is located anteriorly or anterolaterally. [8] Because of the slow growing nature of the tumor, even partial excision would result in significant relief of pain and neurological symptoms. The role of external beam radiation in partially excised tumors is controversial. Owing to concerns of potential malignancy postoperative radiotherapy has been used in patients following partial excision of spinal epidural angiolipoma. [9],[10],[11] Current literature suggests that because of the benign nature of the tumor and very good prognosis, adjuvant radiation should not be used. [12] References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11039f1.jpg] [ni11039f3.jpg] [ni11039f2.jpg] [ni11039f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}