 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
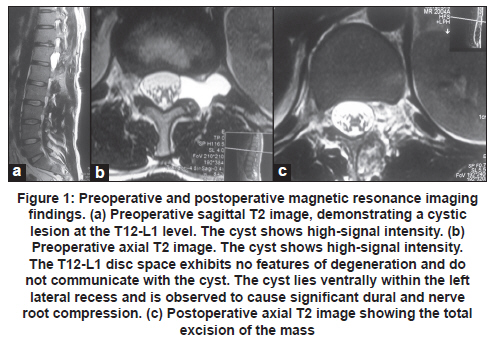
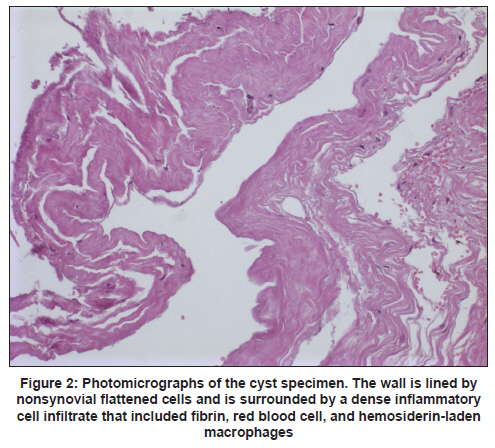
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 136-137 Letter to Editor Ganglion cyst of thoracolumbar region Erdinc Civelek1, Ali Riza Ozcan2, Mehmet Bulent Onal3, Serkan Aydin4, Serap Toru5 1 Department of Neurosurgery, Baskent University Istanbul Hospital, Istanbul, Turkey Extradural cysts within the lumbar spinal canal are usually classified as synovial cyst, posterior longitudinal ligament (PLL) cyst, or ligament flavum (LF) cyst based on their location, [1] origin, [2] and pathologic features. [3] Histological classification includes only true cysts (having synovial membrane) and pseudo cysts or ganglion cyst (no synovial membrane). Almost all LF and PLL cysts are pseudo/ganglion cysts. Ganglion cyst of the PLL of the spine is a rare entity and has no continuity with the facet joint and has no epithelial lining, mostly lumbar and cervical in location. [4] Thoracolumbar location of ganglion cyst has not been documented in the literature. A 25-year-old man with no history of trauma presented with left leg pain which extended from the lateral thigh to dorsum of calf and burning sensation on the left side of chest. The pain was not relieved by analgesics. Neurologic examination was essentially normal except for hyperalgesia in the left T12 dermatome. Magnetic resonance imaging (MRI) revealed a round mass with smooth margins at left T12-L1 level of the spinal canal with no degenerative changes of the spine. The cyst was hypointense on T1-weighted images and hyperintense on T2-weighted images. No cyst-disc communication was apparent on T2-weighted images [Figure - 1]a and b. He had left-sided hemipartial-laminectomy of the T12 and foraminotomy of left L1 root and total excision of the cyst [Figure - 1]c. Macroscopically, a unilocular cyst with a fibrous tissue wall was observed. Histologically, the cyst wall was lined by nonsynovial flattened cells and surrounded by a dense, mononuclear, inflammatory cell infiltrate that included eosinophils and macrophages [Figure - 2]. On the basis of these macroscopic and microscopic results, the diagnosis of a ganglion cyst originating from the PLL was made. At 10 month postoperative follow-up, the patient had full resolution of symptoms. The pathogenesis of the ganglion cysts is not well understood, but may involve repetitive trauma, facet arthrosis, spondylolisthesis, and myxomatous degeneration of the connective tissue, increased hyaluronidase production and accumulation of viscous myxoid material. [5] As in this patient, the ganglion cysts can be congenital. [6] Meningioma, schwannoma, metastatic tumors, disc herniation, and pannus formation due to romatoid arthritis should be considered in the differential diagnosis. Diffuse contrast uptake can be observed in meningiomas. High signal characteristic is present in schwannomas. Metastatic tumors usually cause osteolysis. In romatoid arthritis, physical symptoms predominate. Lumbar disc herniation usually has a signal equivalent to that of the adjacent degenerative disc: i.e., isointense or hypointense on both T1- and T2-weighted imaging. All cysts are hypointense on T1-weighted images, hyperintense on T2-weighted images with a rim of enhancement after gadolinium administration. [7],[8] Spontaneous regression of synovial cysts has been observed. [7] In addition to conservative treatment methods, various minimal invasive methods have been done for lumbar spinal cyst including CT or endoscopy-guided needle aspiration. [7],[8] Surgical treatment is the gold standard, and the cyst wall should be removed to avoid recurrence. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11040f1.jpg] [ni11040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}