 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
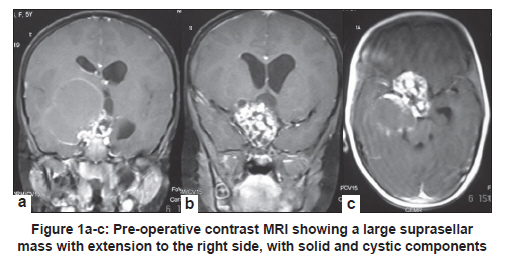
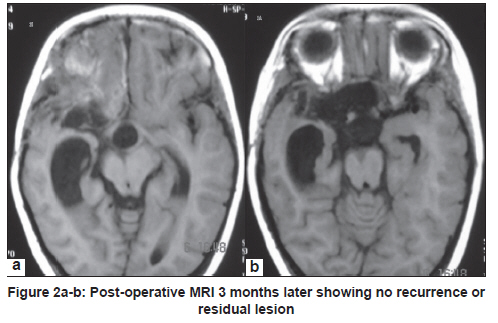
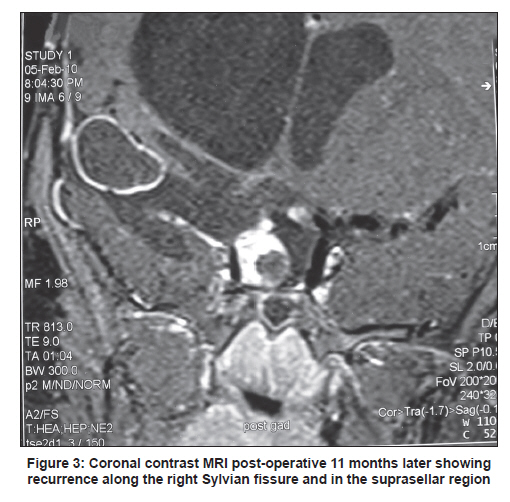
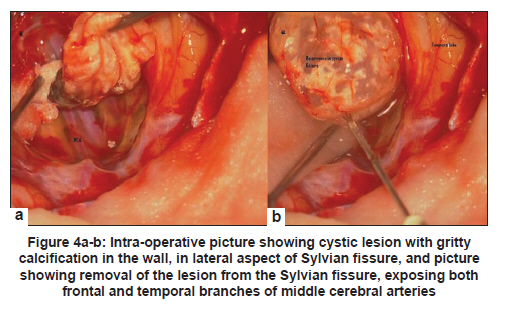
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 137-139 Letter to Editor Ectopic recurrence of craniopharyngioma along the surgical tract Pravin Salunke1, Lalit K Bhardwaj1, Kirti Gupta2, Kajal Das1 1 Department of Neurosurgery, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India Craniopharyngiomas are considered as the most common non-glial intracranial tumours in children. In adults, they account for approximately 2%-4% of brain tumours. Although histologically craniopharyngiomas are benign tumours, they tend to locally infiltrate the surrounding neurovascular structures, making the complete excision challenging. [1] A 5-year-old female child presented with left side weakness and right side progressive loss of vision of 3-month duration. Magnetic resonance imaging (MRI) showed suprasellar enhancing lesion, extending more on the right side [Figure - 1]. She underwent a right frontotemporal craniotomy and near total excision. A branch of right anterior cerebral artery was inadvertently injured during surgery. Fortunately, the patient did not develop new deficits. Follow-up MRI at two months did not show any residual lesion [Figure - 2]. Follow-up MRI after 11 months showed a cystic collection with enhancing wall in the right Sylvian fissure and another lesion along the stalk and suprasellar region with solid and cystic components [Figure - 3]. However, she was asymptomatic. At redo-craniotomy, two cysts were seen in the Sylvian fissure. One cyst had straw-coloured fluid and gritty calcifications and total excision was done [Figure - 4]. Another large cyst was present in the interoptic space and suprasellar region, which also had straw-coloured fluid and calcification and firm solid components. The entire solid component and wall of the cyst was peeled off the arachnoid along the stalk. Postoperatively, she developed diabetes insipidus, which required desmopressin. The follow-up MRI after six weeks showed no recurrence or residual lesion. Histopathology was suggestive of adamantinomatous variety of craniopharyngioma. The MIB index was low. We decided against radiotherapy, considering her age. There are a few reports of ectopic recurrence of craniopharyngiomas, 26 cases till date, including our case. Local recurrence, as high as 25%-70%, has been reported. The most frequent mechanism of dissemination is seeding of tumour cells along the surgical route. During the resection, tumour cells may remain along the operative route and grow. However, the exact mechanisms or surgical techniques predisposing for the ectopic recurrences are unknown. The other proposed mechanism is spillage of tumour cells into the subarachnoid space. This mechanism can explain the ectopic recurrence in the posterior cranial fossa, supratentorial region unrelated to the surgical site and spine in the lumbar region. [1],[2],[3],[4] All ectopic recurrences have been reported in patients who had undergone tumour removal by transcranial approach and no case has been reported after removal by transsphenoidal approach. Literature suggests that even complete resection does not prevent ectopic recurrence. [2] The time between the initial presentation and evidence of ectopic recurrence has been variable and in the range of 1-21 years. [3] The histological characteristics of craniopharyngioma seem to have some bearing on the recurrence, both ectopic and local. The adamantinomatous type is associated with a worse post-operative outcome and has a greater risk for recurrence than the squamous papillary type. [4] Proliferative indices may predict local recurrence. However, its role in ectopic recurrence remains to be determined. [4] Meticulous surgery with careful inspection of surgical field and abundant irrigation is one way to prevent ectopic recurrence. Post-operative radiotherapy, though controversial for patient with total resection, may be an option for preventing ectopic recurrence. Theoretically, radiotherapy can destroy residual tumour cells at the site of resection as well as microdeposits at different sites. [4] However, the ill-effects of radiotherapy should not be underestimated. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11041f4.jpg] [ni11041f3.jpg] [ni11041f2.jpg] [ni11041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}