 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
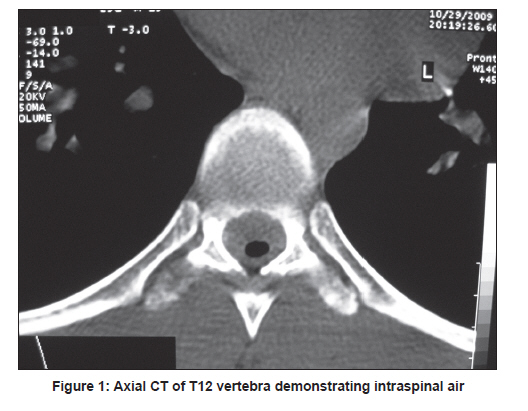
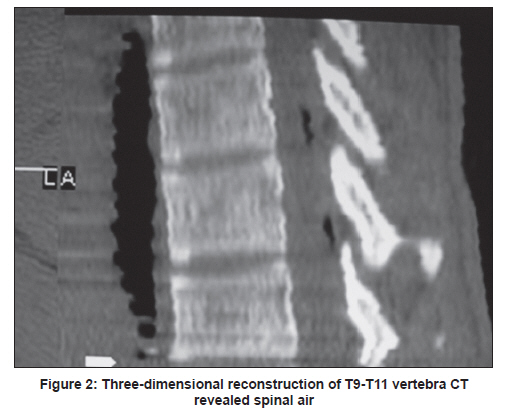
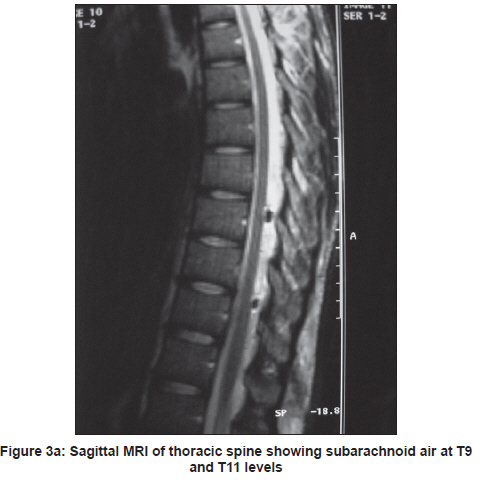
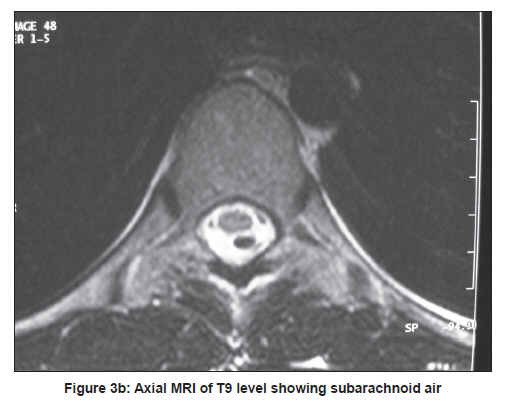
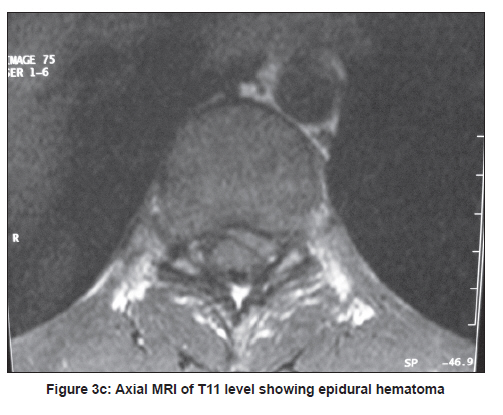
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 139-141 Letter to Editor Isolated subarachnoid pneumorrhachis Habibullah Dolgun1, Bora Gurer1, Onur Sari2, Zeki Sekerci1 1 Diskapi Education and Research Hospital, Neurosurgery Clinic, Irfan Bastug cad. Diskapi, Ankara, Turkey A 19-year-old man was admitted to the emergency department for a stab injury on his back with a knife. Physical examination revealed a 3-cm puncture wound at the level of the T9-T10 vertebrae. Neurological examination was essentially normal. Plain radiographies of the head, chest and spine were also normal. Computed tomography (CT) [Figure - 1], and three-dimentional reconstruction of the thoracic spine CT [Figure - 2] revealed air within the spinal canal at the T9-T11 level. Magnetic resonance imaging (MRI) of the thoracic spine revealed subarachnoid air and also an 4-5-mm epidural hematoma at the T9-T11 level [Figure - 3a, Figure - 3b, Figure - 3c]. CT of the head, thorax and abdomen showed no pathologies. The initial diagnosis was subarachnoid pneumorrhachis and epidural hematoma. Patient was started on antibiotics for the prophylaxis. During the hospital stay there was no neurological deterioration or any development of cerebrospinal fluid fistula. He was discharged on Day 10. The follow-up MRI taken after one month showed resolution of air pact and epidural hematoma. Pneumorrhachis, air in the spinal canal is an unusual condition and only few case reports have been published in the English literature. [1] The most common cause of pneumorrhachis is trauma or iatrogenic manipulations; other rare causes include respiratory complications, malignancies, cardiopulmonary resuscitation, inhalational drug abuse, diabetic ketoacidosis-associated emesis, degenerative disc disease and spontaneous pneumorrhachis. [2] Air within the spinal canal may be seen in the epidural or subarachnoid space; the former is more common, and the latter is extremely rare. [1] Traumatic pneumorrhachis with air in the subarachnoid space is an extremely rare entity and as a rule, is almost always seen in association with air in other body cavities/spaces; pneumocephalus, pneumothorax, pneumomediastium, pneumopericardium or subcutaneous emphysema. [2],[3],[4],[5],[6] Isolated traumatic subarachnoid pneumorrhachis is a unique condition and only one published case of isolated subarachnoid pneumorrhachis of the cervical spine caused by stab wound has been published. [3] Pneumorrhachis is usually asymptomatic and the diagnosis is primarily radiologic. [2] CT is the initial imaging modality; however, detection of air may not be always possible if the air is extradural or intradural. [2] The pressure in the epidural space is much lower than that in the subarachnoid space, by this way, atmospheric air passing through the puncture, then enters to the epidural space. [7] When there is associated arachnoid damage it may then enter the subarachnoid space. Magnetic resonance imaging and intrathecal contrast CT scan are the investigative modalities to detect extradural or intradural air. The limitation of intrathecal contrast CT is that it may be impossible to exclude the possibility of lumbar-puncture-related air in the subarachnoid space. There are no set treatment guidelines as traumatic pneumorrhachis, both asymptomatic and symptomatic, is a rare condition. The presence of pneumorrhachis implies an open injury and is associated with the possible risk of meningitis. The general approach is conservative with meningitis prophylaxis unless there is neurologic deterioration. [8] References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11042f3b.jpg] [ni11042f1.jpg] [ni11042f3a.jpg] [ni11042f2.jpg] [ni11042f3c.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}