 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
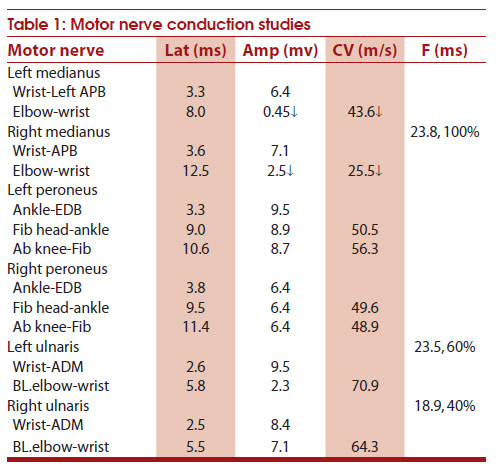
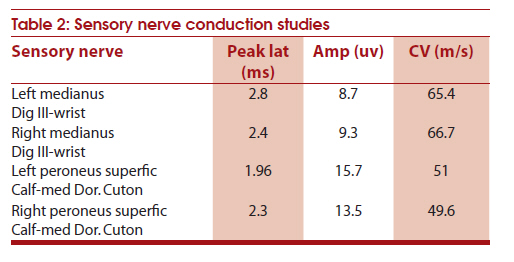
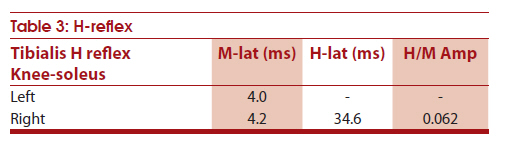
Neurology India, Vol. 59, No. 1, January-February, 2011, pp. 141-142 Letter to Editor Chronic inflammatory demyelinating polyneuropathy following treatment with peglated interferon α-2a for chronic hepatitis C virus infection Chang Ying, Han Xue-mei, Gao Yao, Liu Song-yan Department of Neurology, China-Japan Union Hospital, Jinlin University, Changchun,130033, China The etiopathogenisis of chronic inflammatory demyelinating polyneuropathy (CIDP) is unknown yet. Peglated interferon α-2a is an antiviral biological agent, which is widely used to treat chronic viral hepatitis. Although neurological complications such as myasthenia gravis, axonal neuropathy, and central nervous system demyelination have been reported [1],[2] during interferon-α therapy, CIDP is rarely reported. Here, we report a patient with chronic hepatitis C virus (HCV) infection, who developed CIDP during treatment with Peglated interferon α-2a. A 47-year-old man, who was a diagnosed case of chronic HCV infection in October 2009, was commenced on Peglated interferon α-2a treatment 180 μg subcutaneously once a week in March 2010. After 2 months of antiviral treatment (in May 2010), he developed numbness and weakness of both lower and upper limbs gradually. He received Vitamin B12 treatment, but with no improvement. He discontinued Peglated treatment in June 2010, but his neurological symptoms deteriorated gradually. He presented to us with motor weakness (4/5 grade) of all the four limbs. Deep tendon reflexes were absent. Both hands were dry and rough and hand nails were fragile. Hypoesthesia was noted in the outer part of the lower legs. Cerebrospinal fluid (CSF) was clear, with normal pressure (120 mmH 2 O), 3 leukocytes/mm 3 , normal glucose (4.2 mmol/L) and chloride (120 mmol/L), and elevated protein (2.0 g/L). Nerve conduction studies revealed reduced conduction velocity in both the median nerves, conduction block in both median nerves and left ulnar nerves, prolonged F-wave latency in left ulnar nerve, reduced F-wave frequency in both ulnar nerves, and no H reflex in left tibial nerve [Table - 1],[Table - 2],[Table - 3]. Clinical features, electrodiagnostic studies, and CSF findings supported the diagnosis of CIDP. [3] He was started on intravenous 10 mg/day Dexamethasone treatment for 7 days, followed by 50 mg/day oral prednisone. He did not show any improvement with this treatment for 2 weeks. He was started on intravenous immunoglobulin (0.4 g/kg for 5 days), with which he showed marked improvement in his muscle power over the next 2 weeks. The patient was discharged with nearly normal muscle power. This patient had CIDP and the possible etiology could be the following: HCV infection related, Peglated treatment complication, and Peglated triggered CIDP. Interferon α-2a is a broad-spectrum antiviral agent. The common side effects include fever flu-like symptom, myelosuppression and autoimmune diseases such as thyroiditis, thrombocytolytic, rheumatoid symptoms, systemic lupus erythematosus, type I diabetes.[4],[5],[6],[7],[8] These symptoms subside following the withdrawal of the medicine. Neurological complications such as myasthenia gravis, autonomic neuropathy sensory neuropathy, chronic inflammatory demyelinating neuropathy (CIDP) and acute inflammatory demyelinating neuropathy (AIDP) are rare. Two cases of AIDP have been reported in association with peglated interferon α-2a therapy for chronic hepatitis B and C virus infection.[9],[10] Makoto Hirotai [11] reported one case of chronic HCV infection, who developed weakness and numbness of all the four limbs during treatment with Peglated. The pathogenesis of CIDP is not fully understood; dendritic cells (DCs) probably play an important role in the pathogenesis of CIDP. DCs are antigen-presenting cells (APCs) which play a critical role in the regulation of the adaptive immune response. DCs are unique APCs and only DCs have the ability to induce a primary immune response in resting naïve T lymphocytes. Studies by Salomon et al. [12] suggested that autoimmune diabetes-prone diabetes mouse, deficient in B7-2 costimulation, was protected from developing diabetes but developed spontaneous autoimmune peripheral polyneuropathy. The spontaneous autoimmune peripheral polyneuropathy in these mice had many similarities to CIDP in humans. Press et al. [13] reported the presence of antigen-loaded DCs in the CSF of patients with CIDP. Probably these antigen-loaded DCs then may enter CSF-draining lymphatic vessels and travel to regional lymph nodes, where matured DCs interact with T and B cells to induce and modulate myelin-reactive T and B cell responses, whereas interferon-α could promote maturity of peripheral blood monocyte-derived DCs. [14] These findings suggest that interferon-α probably activates T and B cells via DCs, resulting in CIDP. In conclusion, though rare, interferon-α treatment may cause CIDP. Since interferon-α is widely used for the treatment of chronic hepatitis C and B virus infections, physicians should be aware of the side effect so that an early diagnosis and treatment can be initiated. References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11043t3.jpg] [ni11043t2.jpg] [ni11043t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}