 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
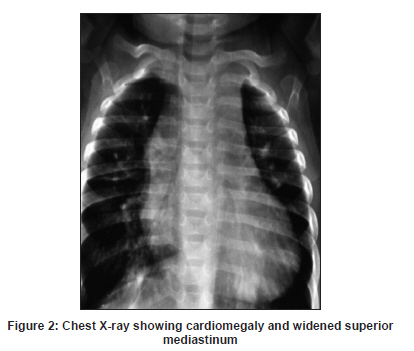
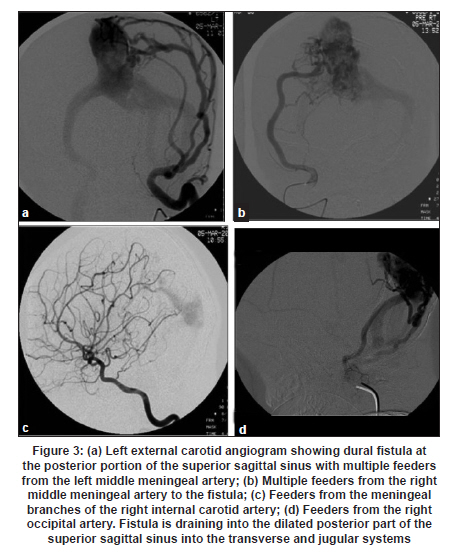
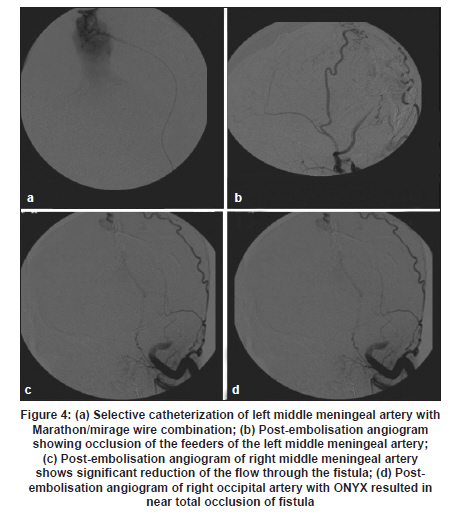
Neurology India, Vol. 59, No. 6, November-December, 2011, pp. 917-918 Letter to Editor Role of endovascular embolisation in treatment of pediatric dural arteriovenous fistula: A case report with a review of the literature Lakshmi Sudha Prasanna Karanam, Sridhar Reddy Baddam, Santhosh Joseph Department of Radiology and Imaging Sciences, Sri Ramachandra University, Chennai - 600 116, India Dural arteriovenous fistulae (DAVF) account for 10-15% of all intracranial arteriovenous malformations and are rare in the pediatric population with a reported incidence of 10%. [1],[2],[3] We describe DAVF in an eight-month-old treated by endovascular embolisation with significant clinical improvement. An eight-month-old male child presented with breathlessness, generalized tonic clonic seizures, and delayed milestones. On clinical examination he had signs of respiratory distress, cardiac murmur and facial nevus with dilated veins, bruit predominantly in the right frontal region [Figure - 1]. Two-dimensional (2D) echocardiogram revealed isolated right pulmonary vein with drainage into inominate vein and dilated cardiac chambers. Chest radiograph [Figure - 2] showed cardiomegaly and widened superior mediastinum. Computed tomogram (CT) of brain revealed dilated ventricular system with avidly enhancing extra-axial lesion in the occipital region. Digital subtraction angiogram (DSA) confirmed the presence of DAVF in the posterior part of the superior sagittal sinus fed by feeders from bilateral occipital, middle meningeal, and superficial temporal arteries with transosseous feeders, pial branches from the left posterior cerebral artery, meningeal branches from internal carotid arteries, leading to a large dilated venous sac situated in the posterior part of the superior sagittal sinus and drains through both transverse, sigmoid and jugular systems [Figure - 3]a-d. There was presence of cortical venous reflux. However, the jugular bulbs were normal. Subsequently, the child was taken up for embolisation, 4F slip catheter was placed in the left middle meningeal artery and feeders were selectively catheterized and embolised with 60% N-butyl cyanoacrylate glue. Similar procedure was done on the right middle meningeal artery. Then the right occipital artery was selectively catheterized with Marathon/Mirage microcatheter/microwire combination and onyx 18 (0.4cc) was injected. Post-procedure angiogram revealed near total obliteration of all the embolised feeders with significant reduction in the shunt, more than 90% [Figure - 4]a-d. The venous drainage was predominantly antegrade. Immediate followup showed that the dilated veins over the right frontal region with bruit had completely subsided and child was relived of respiratory distress. At three months, six months, and one year follow-up there was significant improvement in the child′s clinical status with seizures and cardiac function being well controlled. In children DAVF usually tend to be multifocal and more aggressive as compared to adults. [5] Our present case had a dural sinus malformation. Three types of dural arteriovenous shunts have been described in the pediatric population: (1) neonatal type dural AV shunt, a malformation of dural sinus (DSM), (2) infantile dural arteriovenous shunt, and (3) adult type DAVF. [5] DSM are associated with slow-flow multiple AV shunts within the wall of the dural pouch contributing to venous congestion. The most common symptoms are related to increased intracranial pressure, cardiac failure and coagulation disorders. Infantile shunts usually are multifocal and present with congestive cardiac failure. The natural history includes progressive venous occlusion usually present with well-tolerated congestive heart failure. Treatment is postponed until the development of macrocrania. Cavernous sinus capture determines the development of neurological symptoms which is the natural bypass to the venous outflow. [5,6] Lasjunuias et al., suggested that a primary underlying structural weakness of the dura coincides with a trigger factor resulting in the formation of DAVF. [7] Endovascular treatment of DAVF is lifesaving in the setting of cardiac failure as in our patient. Targeted embolisation at the specific area of shunting should be aimed as proximal embolisation is associated with rate of recurrence. [8] References
Copyright 2011 - Neurology India The following images related to this document are available:Photo images[ni11283f1.jpg] [ni11283f3.jpg] [ni11283f4.jpg] [ni11283f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}