 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
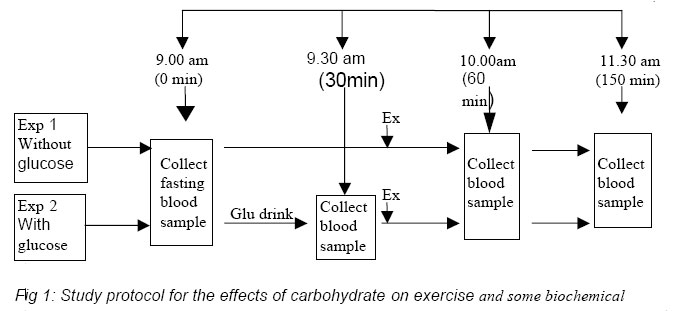
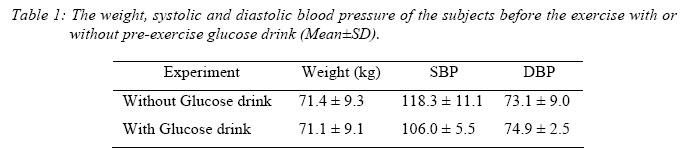
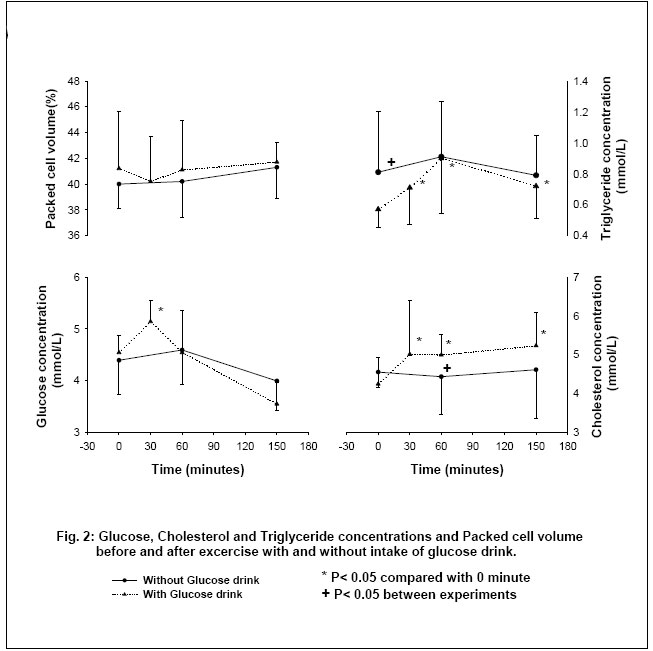
Nigerian Journal of Physiological Sciences, Vol. 20, No. 1-2, 2005, pp. 43-47 EXERCISE PERFORMANCE IN RELATION TO GLUCOSE DRINK AND THEIR EFFECT ON SOME BIOCHEMICAL PARAMETERS. 1,2 S. C. MELUDU *, 3 L. ASOMUGHA, 2 E. C. DIOKA, 3 C. OSUJI, 4 A. C. AGBASI, 5 M. IFEANYICHUKWU AND O. A. OLUBOYO6 Departments of; 1Human Biochemistry, 2Chemical Pathology, 3Medicine, 4Medical Microbiology, 5Haematology and 6Pharmacology, College of Health Sciences, Nnamdi Azikiwe University, Nnewi. PMB 5001, Nnewi. E-mail; Emeka_m@yahoo.com Received:26/4/2005 Code Number: np05008 Summary: This study was designed to determine the effect of glucose drink on marathon running and on some biochemical parameters. Seven untrained athletes (male students) participated in this study and were engaged in marathon running with and without intake of glucose drink (1g/kg body weight) in a double blind procedure. Blood samples were collected at 0, 30, 60 and 150 minutes for serum glucose, triglyceride, cholesterol and PCV estimation. There were significant increases in serum glucose (F=13.01; P<0.01) and triglyceride (F=6.87; P<0.01) following pre-exercise glucose drink, while PCV remained unchanged with or without pre-exercise glucose drink. Greater than 80% of the subjects covered more distance with glucose intake than without glucose drink. It is concluded that carbohydrate intake prior to exercise may enhance exercise performance and spares glycogen and lipid utilization. Key Words: Glucose ingestion, Marathon exercise, Triglyceride, Cholesterol. Introduction Carbohydrate delays fatigue by limiting dehydration, maintaining blood glucose, and spares muscle glycogen (Nikolopoulos et al, 2004, Grimm et al, 2004). Carbohydrate ingestion attenuates the increase in plasma free tryptophan that can limit brain serotonin synthesis and possibly delay CNS fatigue (Gollnick et al, 1974). During high intensity intervals, muscles rely primarily on muscle glycogen as a source of fuel, which can result in glycogen depletion within minutes (Kat et al, 1986; Kuipers et al, 1991). Athletes are therefore advised to consume sufficient amount of carbohydrate prior to exercise in order to optimize muscle glycogen levels (MacLaren et al, 1994). On the other hand, high-fat diet result in low muscle glycogen concentration and utilization (Zderic et 2004). In humans, training reduces the rate of glucose uptake during moderate intensity exercise of maximal oxygen uptake (Coggan et al, 1990). However, the rate of glucose uptake increases exponentially with increasing exercise intensity and trained individuals are capable of exercising at higher intensities than untrained individuals (Jansson and Kaijser, 1987). Furthermore, the rate of glucose uptake by muscle depends on both exercise and circulating insulin concentration (DeFronzo et al, 1979). When the time between carbohydrate ingestion and exercise is less than approximately one hour, hypoglycemia may occur during the first 30 minutes of exercise (Ahlborg and Felig, 1977). This is probably mediated by hyperinsulinaemia and relative hyperglucagonaemia (Ahlborg and Felig, 1977). The necessity of physical exercise for the prevention of and treatment of hyperlidaemia is well known. It is recognized that long-term exercise contributes to lowering of VLDL-TG and Cholesterol (Carlson and Mossfeldt, 1964), and contributes to higher concentration of HDL-cholesterol, which is considered to have anti-atherosclerotic action (Deshaies et al, 1983). In this study, we investigated the effects pre-exercise intake of glucose drink on exercise performance, blood glucose and lipid levels and packed cell volume. Materials and Methods Seven healthy untrained medical students aged (21.9±1.7 years; range 20-24 years) participated in the study after they gave their informed consent. The study involved marathon running, and half of the subjects alternated between running after glucose drink (1g/kg body weight of pure Glucose (BDH Chemicals, England) dissolved in 250 ml of water) and without glucose drink. This protocol was repeated after a week interval. They were all placed on the same diet 24 hours prior to the days of exercise. On each day of exercise, they arrived at the laboratory after an overnight fasting and their weight, height and blood pressures were taken (see protocol in figure 1). The subjects underwent 30 minutes of marathon race, thought some of them tired out before the end of the race. 10 ml of blood samples were collected at different time interval as indicated in the protocol and placed in plain tubes for the determination of serum glucose, triglyceride and cholesterol and in EDTA tubes for determination of PCV. The serum was separated, and serum glucose determined afterwards, while serum for triglyceride and cholesterol was stored frozen until analyzed. Serum glucose was determined by glucose oxidase method (Sheiko et al, 1979), triglyceride by colorimetric method after post-enzymatic hydrolysis with lipase (Bucolo and David, 1973) and cholesterol determined after enzymatic hydrolysis and oxidation (Pearson et al, 1953) using Randox test kits. PCV was determined by microhematocrit method. Statistical Method: ANOVA was used to test for differences for repeated measure and student t-test for paired samples was applied to test for difference between measures. Significant level was accepted at P< 0.05. Results In all subjects there was no significant change in weight, and diastolic blood pressure (DBP) of the subjects at the time of the two experiments. However, there was a significant change in systolic blood pressure (SBP) of the subjects at the time of the two experiments (P<0.05) (Table 1). Following pre-exercise glucose drink, serum glucose level increased significantly at 30 minutes compared with zero minute (51.4±0.41 vs 4.54±0.33 mmol/L; P<0.05). Afterwards, the value at 60 minutes (4.54±0.82 mmol/L) and 150 minutes (3.54±0.42 mmol/L) returned to the pre-glucose drink level (Figure 2). On the other hand, there was no significant change in the serum glucose levels of the subjects following exercise without pre-exercise glucose drink. Furthermore, glucose levels at different time intervals were not significantly different with or without pre-exercise glucose ingestion, but at 150 minutes the value though not significant, was much decreased with pre-exercise glucose drink (Figure 2). There was a significant change in serum triglyceride concentrations with pre-exercise glucose drink (F=6.87; P<0.01). In fact, serum triglyceride concentration increased significantly from the value at 0 minute (0.57±0.12 mmol/L) and remained increased even at 150 minutes (0.72±0.21 mmol/L; P<0.05) (Figure 2). On the other hand, there was no significant change in serum triglyceride levels following exercise without pre-exercise glucose ingestion. We however, did observe a significantly elevated fasting serum triglyceride level in the subjects on the day of exercise without pre-exercise glucose ingestion when compared with pre-exercise glucose ingestion (0.57±0.12 vs 0.81±0.38 mmol/L; P<0.05) (Figure 2). Following pre-exercise glucose drink, serum cholesterol concentrations increased significantly from the value at 0 minute (4.24±0.70 mmol/L) and remained elevated at 150 minutes (5.23±0.85 mmol/L; P<0.05). Serum cholesterol concentration remained unchanged without pre-exercise glucose drink (Figure 2). We however observed a significantly higher serum cholesterol value with pre-exercise glucose ingestion compared with without glucose ingestion at 60 minutes (4.99±0.54 vs 4.43±0.97 mmol/L; P<0.05) (Figure 2). There was no change in packed cell volume (PCV) following exercise with or without pre-exercise glucose drink and when both are compared together (Figure 2). However, subjects covered more distance after pre-exercise glucose ingestion when compared with distance covered without pre-exercise glucose ingestion (6008.6±1397.2 vs 4947.1±1036.8m; P<0.05). Discussion In normal subjects after an oral glucose tolerance test, the blood glucose value after initial increase is expected to return to nearly pre-glucose ingestion value after 60 minutes. This was the case in this study as serum glucose value after 60 minutes was decreased after the initial increase at 30 minute. We however observed that exercise could also have contributed to this decrease in serum glucose level. In fact, it has been shown that when the time between carbohydrate ingestion and exercise is less than approximately one hour, hypoglycemia may occur during the first 30 minutes of exercise (Ahlborg and Felig, 1977). Though that was not the case in this study, but there was the tendency for hypoglycemia to occur following pre-exercise glucose ingestion compared with without pre-exercise glucose ingestion (Figure 2). In support of the reports that the rate of glucose uptake by muscle depends on both exercise and circulating insulin concentration (DeFronzo et al, 1979), we are of the opinion that the consequent insulin release followed with exercise contributed to lowering of serum glucose level with pre-exercise glucose ingestion. The necessity of physical exercise for the prevention of and treatment of hyperlidaemia is well known. It is recognized that long-term exercise contributes to lowering of VLDL-TG and Cholesterol (Carlson and Mossfeldt, 1964), and contributes to higher concentration of HDL-cholesterol, which is considered to have anti-atherosclerotic action (Deshaies et al, 1983). On the contrary, there was an increase in serum triglyceride in the subjects after pre-exercise glucose drink. Similarly, there was a sustained rise in serum cholesterol level following exercise after pre-exercise glucose ingestion unlike in the subjects after exercising without glucose ingestion. The increase in serum triglyceride levels in subjects following exercise after pre-exercise glucose drink could probably be due to the fact that the body spared fat stores in the presence of glucose. The inability of one subject to maintain a fasting state prior to exercise without glucose ingestion, probably resulted in a higher fasting serum triglyceride concentration in the subjects prior to exercise without glucose ingestion compared with glucose ingestion. Normally, prolonged exercise should cause an increase in the level of plasma catecholamines, growth hormone, glucagon and a concomitant reduction in insulin. These changes encourage the release of free fatty acid from triglyceride stores and their subsequent use as energy source (Davis et al, 1992). In this study, the subjects are untrained athletes and are hardly engaged in exercise. It is therefore unexpected that the change in triglyceride and cholesterol associated with long-term exercise were not observed. The fact that there was no change in packed cell volume (PCV) with or without pre-exercise glucose ingestion followed with exercise, showed that the plasma volume was not changed by exercise performance and hence the changes in the concentrations of the assayed parameters reflected the actual change brought about by either exercise or glucose ingestion. The difference in SBP between the two experiments in the subjects could probably be due to anxiety on the part of some subjects. As expected, there was no change in the weight of the subjects between the two experiments, since the time interval for a noticeable change in weight was just one week and therefore very small. It seemed that fatigue was delayed by the ingestion of carbohydrate, and may explain more distance covered by the subjects after pre-exercise glucose drink. In fact, carbohydrate ingestion was shown to limit dehydration, maintain blood glucose level and spares muscle glycogen (Gollnick et al, 1974). In conclusion, our work suggest that glucose ingestion could be of value in enhancing exercise performance by delaying fatigue in addition to maintaining blood glucose concentration and sparing blood lipids. Acknowledgement We are very grateful to the Medical Students’ Research Goup (MESREG) of College of health Sciences, Nnewi and in particular to Abone S, Okey-Umeh U, Eleje G, Nwankwo A, Unigwe S and Obiesie A for their great contibution, which made the study possible. We are also grateful to all our student volunteers. We thank you all. References
© Physiological Society of Nigeria 2005 |

{kind=link}
{kind=link}
{kind=link}