 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
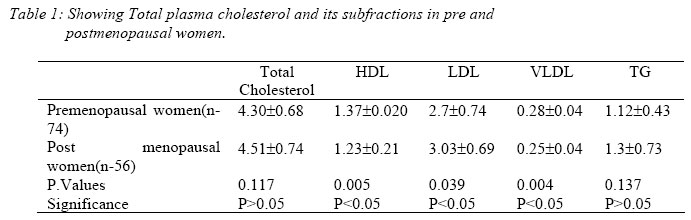
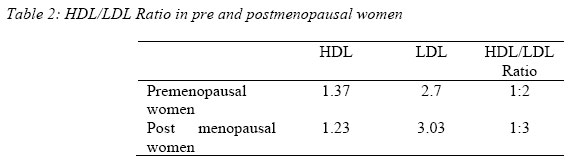
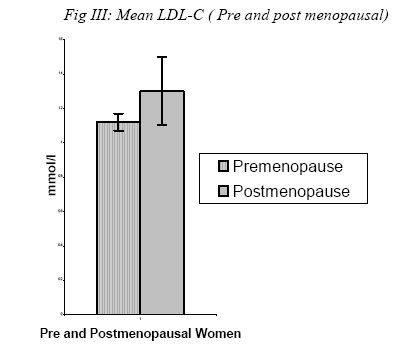
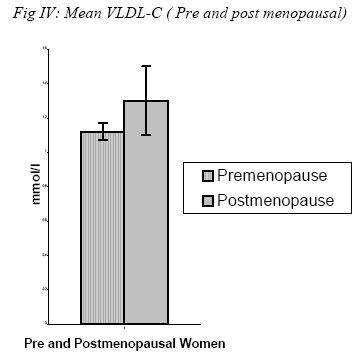
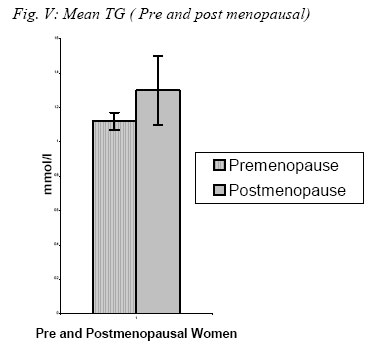
Nigerian Journal of Physiological Sciences, Vol. 20, No. 1-2, 2005, pp. 48-53 THE EFFECTS OF MENOPAUSE ON THE SERUM LIPID PROFILE OF NORMAL FEMALES OF SOUTH EAST NIGERIA J. C. IGWEH1, I.U. NWAGHA1, J. M. OKARO 2 1Department of Physiology, Faculty of Medicine, College of Medicine, University of NigeriaEnugu Campus, EnuguNigeria.2Department of Obstetrics and Gynaecology, Faculty of Medicine, University of Nigeria, Enugu Campus, EnuguNigeria.. Email: jcigweh@yahoo.com, Tel: +234 8033 247 168 Received:22/3/2005 Code Number: np05009 Summary: Dyslipidemia in menopause is a known feature in women, whether it leads to significant increase in the development of coronary heart disease (CHD) is still controversial, more so in our environment where little work has been done. The present study is aimed at comparing the level of total serum cholesterol, including its subunits in premenopausal with that of their postmenopausal counterparts. This is to enable us ascertain the relative risk of developing cardiovascular disease in postmenopausal women in our environment. One hundred and twenty six (126) apparently healthy, non-pregnant females (74 premenopausal and 52 postmenopausal) were recruited for the study. Serum total cholesterol and their subfractions- high-density lipoproteins (HDL), low-density lipoproteins (LDL), very low-density lipoproteins (VLDL) and triglycerides (TG) were estimated using enzymatic and established mathematical methods. There was no significant difference in the total serum cholesterol and triglyceride between the two groups. There was however, a significant reduction of HDL and VLDL in the postmenopausal group (P<0.005) and a significant increase in the level of LDL in the postmenopausal group (P<0.005). The elevated LDL and the reduction of cardio protective HDL and VLDL is an indication that menopause is an independent risk factor for developing cardiovascular disease in our environment.Key Words: Menopause, Dyslipidemia, Cholesterol Introduction Cardiovascular disease is a leading cause of death among women in the developed world. In the United States, more than 500,000 women die of cardiovascular disease and about half are due to coronary artery disease (CAD) (Ariyo et al, 2002). Multiple risk factors have been identified as contributory to the development of CAD. These risk factors are important in both men and women and are present in both Caucasians and Africans. They include cigarette smoking, hypertension, Diabetes mellitus and hypercholesterolemia. Hypercholesterolemia is a key factor in the pathophysiology of artherosclerosis (Igweh et al, 2003). Thus dyslipidemia can be modified by efforts aimed at cholesterol reduction ( Fick et al, 1987, Kane et al, 1990, Davidson 1993). Studies have shown that women are at less risk of developing CAD than their male counterparts, but this is abolished after 60 years of age (Rich-Edward 1995 et al, Courderc et al, 1999). High levels of LDL and low levels of HDL are strongly associated with the risk of CAD ( McNamara et al 1992). Smaller LDL particles (LDL-III) are considered more atherogenic than larger more buoyant species because of their increased susceptibility to oxidation ( Dejagar et al, 1993) and their increased residence time in plasma (Rainwater, 2000). Plasma triglycerides concentration also has a determinative influence on the concentration of small dense LDL particles in normal population (Dejagar et al, 1993, Mendelsohn, 1999). After menopause, there is loss of ovarian function. This results in adverse changes in glucose and insulin metabolism, body fat distribution, coagulation, fibrinolysis and vascular endothelial dysfunction (Spencer et al, 1977). There is also derangement of lipoprotein profile independent of age (Bales, 2000). A number of changes that occur in the lipid profile after menopause are associated with increased cardiovascular disease risk. Lack of estrogen is an essential factor in this mechanism. Apart from maintaining friendly lipid profile, estrogen changes the vascular tone by increasing nitrous oxide production. It stabilizes the endothelial cells, enhances antioxidant effects and alters fibrinolytic protein (Taddec et al, 1996). All these are cardioprotective mechanisms, which are lost in menopause. Dyslipidemia at menopause is not restricted to Caucasians. It is also evident in women of South Eastern Nigeria. These studies were aimed at determining the degree of dyslipidemia in the women of this region and relate it to the risk of developing cardiovascular diseases. It also attempted to suggest possible methods of reverting to lipid friendly status. Materials and Methods A group of 126 women, 74 premenopausal aged between 25-45 years and 52 postmenopausal aged between 55-70 years were studied. They were of the same social class and selected from workers and students of the University of Nigeria and the University of Nigeria Teaching Hospital (UNTH) community. Some of the postmenopausal women were relatives of the workers. They were randomly selected by a lucky dip of yes or no after an informed consent and ethical clearance from the relevant ethical committee of UNTH Enugu was obtained. Exclusion criteria include obesity, pregnancy, diabetes mellitus, hypertension, hormonal contraception and heavy exercise. Fasting venous samples (10ml) were collected in heparinized bottles. This however, was done on the 7th day of the L.M.P. for the premenopausal group. Sample was centrifuged and plasma separated and stored in plastic tubes at 4oC. Total cholesterol was measured using established enzymatic methods of Allain et al (1974) with the Randox cholesterol kit (Randox England). HDL-C was isolated by HDL-C precipitant method (Lopes-virella et al, 1977). LDL was calculated with a formula from total cholesterol and triglycerides (Friedwald, 1972). Triglyceride was isolated enzymatically as described by Henry (1991) and the expert panel on detection, evaluation and treatment of high blood cholesterol in adults (Expert Panel, 1988). VLDL was calculated using the formula VLDL-C = TG/2.825mmol/L (Henry, 1991). Statistical analysis was done using Excel. Showing the mean and standard deviation. Comparison of mean was by student t-test. Permission was obtained from the Faculty Ethics committee to carry out this experiment. ResultsThe mean, Standard deviation and the P-values for total cholesterol, HDL-C, LDL-C VLDL-C and Triglycerides are shown in Table 1. There was no significant difference in the total cholesterol and the triglycerides between the two groups (P>0.005). However there was significant reduction in HDL and VLDL-C fraction in the postmenopausal group and a significant increase in the value of LDL-C (P<0.005). Table 2 shows the HDL/LDL ratio between the two groups. Figs 1,2,3,4, and 5 represent comparisons of means between the two groups. The mean age for premenopausal women is 36.7±4.74 and that for post menopausal women is 60.9±9.9 Discussion
There are variations in lipid levels obtained in different individuals based on race, age, sex, obesity, exercise, smoking, alcohol, diet, diseases like hypertension, chronic liver and renal diseases (Gordon et al, 1987, Jarikre et al, 2000). However, in this study we tried to exclude the co founding variables and results obtained can be taken as the standard normal in our environment. The premenopausal values are similar to values obtained in other studies in different parts of the country (Ajose et al, 2002, Igweh et al, 2003). However, there is paucity of literature in postmenopausal values in Nigeria, but studies on total cholesterol alone done in Ibadan showed no significant change ( Otolorin et al, 1989), as was the case in our study. Studies in some centers in developed countries showed higher values with dyslipidemia being taken as cholesterol > 240mg% (6.21mmol/l) and occurs in 25-33% of women (Grundy, 1994, Gordon et al, 1989). As a result of racial, genetic and technical differences, it has been suggested that our own cut off level should be adjusted to suit our peculiar circumstances. In determining the risk of cardiovascular disease, the absolute cholesterol value is not the most important factor; rather the concentrations of the various subclasses of cholesterol. In the present study there was no significant differences in the total cholesterol level but there was significant reduction in the cardio protective HDL-C and VLDL-C and significant increase in the artherosclerotic LDL-C. This is in agreement with findings in other studies ( Jenson et al, 1990, Edr et al, 1982, Igweh et al, 2003). It has also been estimated that for any 1mg/dl (0.026mmol/ml) increase in HDL-C, there is a 3% decrease in risk of coronary artery disease and a 4.7% decrease in the risk of mortality from cardiovascular disease (Okonofua 1990). In this study this protective effect was lost by five fold. Again the HDL/LDL ratio was increased in the post menopausal group and it has been shown that HDL/LDL ratio is a significant predictor for the development of artherosclerosis both in Caucasians and Nigerians (Aina 1992, Park et al, 2000). There is no doubt from this study that the changes that occur in the lipid profile after menopause is not friendly for the cardiovascular health of our women. It is generally believed that postmenopausal symptoms are less in our women than their Caucasian counterparts. This may not be true because several studies in the past have shown psychological, physical, biochemical, hormonal and vasomotor parameters that are not of great variance with what is obtained else where (Grundy, 1994, Mandel et al, 2002, Pirway et al, 2002). The problem is that the harsh climatic and poor socioeconomic environment overwhelms our women that they hardly ever complain about menopausal symptoms unless it is severe. The elevated LDL and the reduction in the cardio protective HDL and VLDL is an indication that menopause is an independent risk factor for developing cardiovascular disease in our environment. Several studies have shown the beneficial effects of hormonal replacement therapy on the lipid profile of menopausal women (Abbot et al, 1988, Stampfer et al, 1991, Stampfer, 1991). However, controversy exists as to whether these changes culminate to reduced risk of cardiovascular heart disease. Observational studies over the years have touted the beneficial effects of hormone replacement therapy (HRT) in preventing coronary heart disease in post menopausal women (Hulley et al, 1998). More recent studies have however, cast some doubts on the beneficial effects of HRT especially in patients with established cardiovascular disease (Cheng, 2000). Further studies are needed in this area. It should be noted that our post menopausal women have unfriendly lipid profile; it is thus important to note this and device means of correcting the dyslipidemia since the use of HRT and lipid lowering drug is still controversial. It is important to counsel on proper dietary, social and physical habits. References
© Physiological Society of Nigeria 2005 |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}