 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
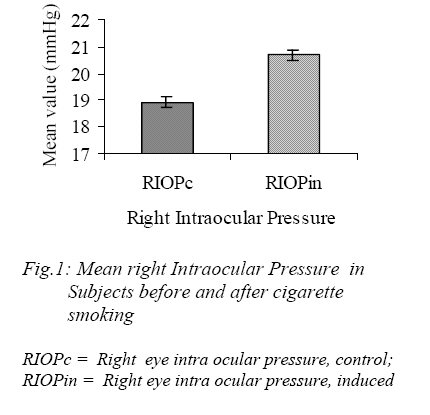
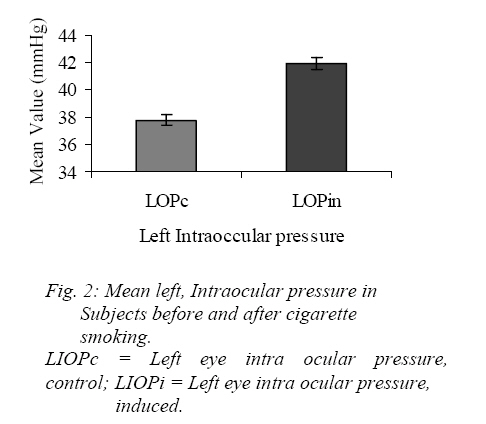
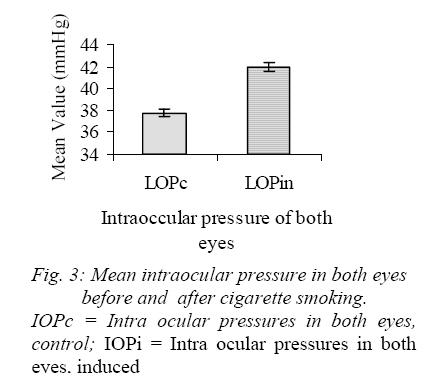
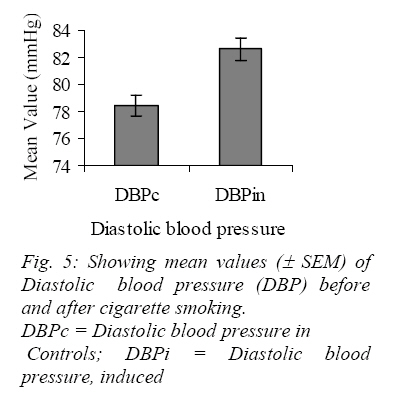
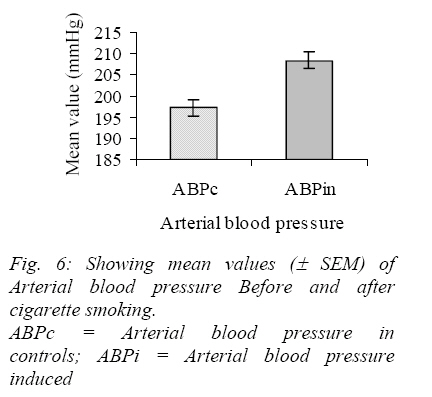
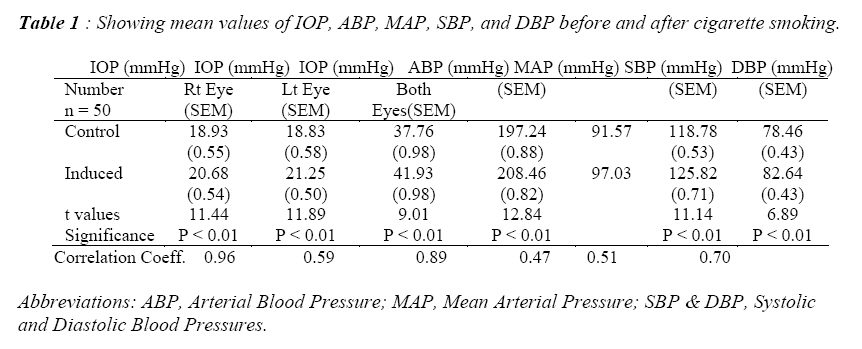
Nigerian Journal of Physiological Sciences, Vol. 22, No. 1-2, 2007, pp. 31-35 The Effects of Cigarette Smoking on Intraocular Pressure and Arterial Blood Pressure of Normotensive Young Nigerian Male Adults C. O. Timothy and R. O. Nneli* Ocular Physiology Unit, Department of Optometry and * Department of Physiology, College of Medicine and Health Sciences, Abia State University, P.M.B. 2000, Uturu, Abia State, Nigeria. Email: emonsly@yahoo.com T el:+ 234 803 087 7004, +234 804 525 6167. Received: 23/10/2006 Code Number: np07005 Summary This study was designed to determine the effects of cigarette Smoking on intra ocular pressure and arterial blood pressure of normotensive young male adults. Fifty male students (who met the screening conditions and devoid of obvious ocular pathology and systemic diseases and non-smokers) had their intra ocular pressure (IOP) measured with a schiotz tonometer and blood pressure(BP) measured with standard syphgmomanometer respectively prior to smoking of two sticks of cigarette each day for one month and thereafter. The result showed a significant (P< 0.01] effect on the intra ocular pressure with a mean control of 37.76±0.98 for both eyes and test of 41.93±0.98. Cigarette smoking increased the blood pressure from mean control of 197.24±0.88 to 208.46±0.82. The increase of both intra ocular pressure and arterial blood pressure was due to nicotine, the principal constituent of cigarette. It is recommended that health care workers should check regularly the IOP and BP of their cigarette smoking patients for early diagnoses of ocular hypertension (glaucoma) and hypertension. Key Words: Cigarette smoking, intra ocular pressure (IOP), arterial blood pressure (BP), ocular, hypertension. Introduction Nicotine is a primary active ingredient of tobacco (Goldfrank et al, 1980). Benowitz (1986) showed that nicotine stimulates the release of norepinphrine and partially accounts for the stimulatory effect of the drug. At a dose absorbed by a typical cigarette smoker, the effect seemed to be on the central nervous system activity while at higher doses, they are direct effect on the nervous system (Benowitz 1986). Normal intra ocular pressures (IOPs) have been reported to vary in both eyes even in the same individuals (Cradle 1940). USPHHS (1997) reported that the smoking prevalence among all respondents were consistently highest for individuals of 18 years or older who were unemployed while education showed a negative correlation with age, that is as years of education goes up, the prevalence goes down among the 18 – 34 years old. Different studies have reported on different values and ranges as the normal values of intra ocular pressure (IOP) as it varies from individuals to individuals. Thus an IOP could be high in one individual but be normal for another (Obubenne1997, Schwabs 1999). Schwabs (1999) reported that 95% of young adults had IOPs range from 10 – 21mmHg which was considered standard value for normotensive young adults. Hence, a deviation from this range either above or below implied ocular hypertension or hypotension. According to Basic Eye Health (2005) toxins associated with smoking may decrease blood flow or cause clot to develop within eye capillaries thus cutting off vital nutrients essential to health. Smoking also caused the development of fragmented molecules known as free radicals which could disrupt normal function of otherwise healthy cells and lead to eye diseases. Smoking may be a risk factor in cataracts, diabetic retinopathy, glaucoma, graves ophthalmopathy and optic neuritis (Basic Eye Health, 2005). Glaucoma, a resultant effect of increased IOP irrespective of its prevalence, remains a multifactorial optic neuropathy of unknown aetiology and inadequate treatment (Tielsch et al, 1995). A reduction in IOP is beneficial to the glaucoma patient ( Heyl et al, 2002 ). Increased blood pressure for months could also damage blood vessels in the heart, the kidneys, the brain and the eyes (Simon and David, 2002). There was a higher prevalence of systolic hypertension in individuals between the ages of 50 – 59 years while high diastolic pressure was a strong predictor of heart attack and stroke in young adults and people of any age with essential hypertension (Simon and David, 2002). Clinically, arterial blood pressures are routine measurements that reflect the status of the cardiovascular system (Kannel, 1976). Thus, the objective of this study was to determine the effects of cigarette smoking on intra ocular pressure and arterial blood pressure on normotensive young male adults in the light of paucity of the former and to correlate the consequence of the presence of both at the same time in the same individuals to health status. Materials and Methods 50 male students of Abia State University, Uturu aged between 18 – 30 years old were recruited for this study after informed consent was sought and obtained from each of them. They were non – smokers whose extensive case history and examination ruled out any previous ocular pathology or systemic diseases, that is, they were apparently healthy subjects who fed three times a day. The measurements of the blood pressure and intra ocular pressure were carried out in the Optometry Clinic of Abia State University, Uturu. The study lasted for one month and between 8.00am –12.00pm. Measurement of Intra ocular and arterial blood pressures All the subjects were allowed to rest for 30 minutes in comfortable chair before the determination of blood pressure. In all subjects, the systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured using mercury sphygmomanometer (Chien, 1977). The blood pressure was taken three times and average served as the mean control blood pressure for the subjects. The intra ocular pressure was measured by using the Schiotz tonometer. The subjects were in a supine position on an examination table and a drop of 0.4 % of Novesin (oxybuprocaine anaesthetic agent) was instilled on the cornea. The instrument was dismantled, cleansed with methyl alcohol to ensure free movement within the shaft. This was tested by placing the footplate centrally on the testing metal block to ensure free pointer movement. The IOP measurement proceeded once the subject indicated that the stinging effect of the anaesthetic drug has stopped. Procedure The subject closed his eyes and the investigator carefully opened the eye to be measured with the left hand such that the thumb held the lower eyelid down and the finger held the upper eyelid so as not to apply pressure which could artificially increase the IOP. The right hand held the tonometer by the handle such that the wing lied between the index and the second fingers respectively, and the other wing held with the thumb, the scale reading was adjusted to face the investigator’s view while he stood behind the subject’s head on side to be measured. The subject was asked to raise the opposite hand directly in front of him and to maintain a fixation at the thumb so that the cornea was exposed with minimized movement during the measurements. The instrument was gently lowered for the footplate to rest squarely on the cornea. The handle was depressed downwards and the reading on the scale which indicated the displacement of the pointer was taken. This was converted to mmHg using a scale provided by the manufacturer. The procedure was repeated thrice and the average served as mean control for each subject. Trial cigarette smoking procedure After the intra ocular and blood pressure were taken inside the clinic, the subjects were taken outside the clinic for cigarette smoking exercise. One stick of Benson and Hedges brand of cigarette was given to each of the subjects to smoke and gulp the smoke at their own pace but simultaneously. The trial cigarette smoking exercise was done for two days to enable the subjects adjust to cigarette smoking and gulping of the smoke as novices. Test (Induced) Measurements After adjusting to cigarette smoking, each of the subjects were given 56 sticks of Benson and Hedges brand of cigarette to be smoked at a rate of two sticks per day at 3 hours intervals for a period of 1 month. The subjects were monitored on a daily basis to ensure compliance to the smoking procedure, and for the intra ocular pressure and blood pressure measurements which were done daily for 1 month for each subject. The average values served as the mean test (induced) for each subject. Average values served as the mean test (induced) for each subject. Statistical Analysis All analyses were done using the SPSS software package. The mean values, percentages, standard error of mean (SEM), t-values of indices were determined and calculated. Values obtained were compared with that of the control values and paired student’s t – test including Pearson’s correlations were used to determine the level at significance at p < 0.01. Results The mean values, standard error of mean and the t–values for the intra. Ocular pressure of the right eye, left eye, both eyes and the arterial blood pressure; systolic and diastolic pressure of the subjects are shown in Table 1. There was a strong correlation coefficient of r=0.96 between intra ocular. Pressure and cigarette smoking using the Pearson’s correlation for the right eye (Fig.1). Cigarette smoking had a strong effect on the IOP of the left eye with a significant difference between the control and experimental values (P < 0.01) (Fig.2). Cigarette smoking also had effect on the IOP of both eyes of the subjects (P < 0 .01) (Fig.3). Cigarette smoking increased the systolic blood pressure (SBP) of the test group over the control (P < 0.01) (Fig.4). There was an increase in the diastolic blood pressure (DBP) after cigarette smoking (P<0.01). However, there was no relationship between cigarette smoking and diastolic pressure using the paired correlation (Fig.5). The mean effect of cigarette smoking on the arterial blood pressure was significant (P< 0.01)(Fig.6). The induced blood pressure was closely related with the control blood pressure(r=0.47) while the correlation coefficient for the systolic and diastolic pressures were 0.51 and 0.70 respectively (Table 1). The correlation coefficient between the induced intra ocular pressure and the control was strong(r=0.89). The degree of correlation for the right eye and the left eye were r=0.96 and r=0.59 respectively. The correlation test showed a direct correlation between intra ocular pressure and arterial blood pressure of the subjects after cigarette smoking. Discussion Mead and Zimmermann (2003) observed a significantly higher effect of cigarette smoking on arterial blood pressure and heart rate in smokers aged 18 – 25 years. Our present findings revealed that cigarette smoking increased both the arterial blood pressure and the systolic blood pressure in normotensive young male adults and hence agreed with the findings of Mehta et al (1998) among smokers and non-smokers. Our control mean arterial pressure and diastolic blood pressure for the normotensive young male adults in university environment corresponded with those non- smokers obtained by Umahi (2004) in residents of Ebonyi State while the control systolic blood pressure for our subjects were lower than those of Umahi (2004) owing probably to the other environmental risk factors like granite dust, effects of rock blasting, chipping dusts inhaled continuously, gold mining dust, salt and salty water intake known to affect arterial blood pressure (Gibbs et al 2000, Mehta et al 1998; Sofola and Obiefuna 1991; Graudal et al 1991). Our results for induced mean arterial pressure, systolic and diastolic pressures corroborated the report of Umahi (2004) for smokers however their systolic pressure was significantly higher than in the present study. This outcome was probably due to the chronic effects in addition to the environmental factors. The mean diastolic pressure was also increased thus indicating a direct relationship between cigarette smoking and cardiovascular parameters. Furthermore, the results suggest that people who indulged in cigarette smoking have increased tendency of developing hypertension and hence, higher diastolic pressure remain a strong predictor of heart attack and stroke in young adults and people of any age with essential hypertension (Simon and David 2002). Our results corroborate the hypothesis that high blood pressure could be caused by cigarette smoking or increases in arterial blood pressure was triggered by cigarette smoking (Gernardt et al 1999). The observed increase in intra ocular pressure due to cigarette smoking was consistent with the report among smokers and non –smokers alike (Okoro 2004). Several workers have demonstrated a IOP in animals with sanguinarine and its alkaloids(Leach, 1955; Hakim ,1954), hence a possible hypersecretory role for cigarette containing nicotine. It has been suggested that increased IOP was observed for the change in the mean values monocularly (that is, it was different for each of the two eyes, and binocularly for the two eyes) for the subjects. This, therefore suggests a relationship between cigarette smoking and intra ocular pressure. The sudden increase in IOP of normotensive subjects after smoking cigarette showed that it could be an important risk factor in the occurrence of glaucoma and ocular hypertension including other chronic ocular diseases such as cataract, macular degeneration (leading to severe visual impairment and blindness), retina ischaemia, anterior ischaemic optic neuropathy, gravis ophthalmopathy, and amblyopic strasbismus (Solbery et al, 1998). The increase in intra ocular pressure and arterial blood pressure obtained after smoking cigarette in the normotensive young male adults was consistent with an association between the degree of arterial blood pressure and the degree of intra ocular pressure already established (Barclays 2004). It is concluded that cigarette smoking disposes the users whether in acute or chronic to systemic ailments and ocular diseases. References
©Physiological Society of Nigeria, 2007 The following images related to this document are available:Photo images[np07005t1.jpg] [np07005f4.jpg] [np07005f3.jpg] [np07005f1.jpg] [np07005f2.jpg] [np07005f6.jpg] [np07005f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}