
|
African Journal of Neurological Sciences
Pan African Association of Neurological Sciences
ISSN: 1015-8618
Vol. 20, Num. 1, 2001, pp. 8-12
|
African Journal of Neurological Sciences, Vol. 20, No. 1, 2001, pp. 8-12
NEUROEPIDEMIOLOGY OF KONZO − A SPASTIC PARA/TETRAPARESIS
OF ACUTE ONSET IN A NEW AREA OF THE DEMOCRATIC REPUBLIC OF CONGO
DESIRÉ TSHALA-KATUMBAY1,3, JEAN-PIERRE
BANEA-MAYAMBU2, THEODORE KAZADI-KAYEMBE1, RAPHAËL
NUNGA-MATADI2, FIDÈLE BIKANGI-NKIABUNGU2, KARIN
EDEBOL EEG-OLOFSSON3, THORKILD
TYLLESKÄR4
1 Centre Neuropsychopathologique du Mont-Amba (CNPP), Université
de Kinshasa, République Démocratique du Congo (RDC)
2 Centre National de Planification de Nutrition Humaine (CEPLANUT),
RDC
3 Department of Neuroscience, Clinical Neurophysiology, and 4
Department of Medical Sciences, Uppsala University Hospital, Uppsala, Sweden
Correspondence to: Desiré Tshala-Katumbay, MD, Department of Neuroscience,
Section for Clinical Neurophysiology, SE - 751 85, Uppsala, Sweden. E-mail:
desire_tshala@yahoo.com
Code Number: ns01003
ABSTRACT
Background:
Konzo is an acute non-progressive spastic paraparesis associated with a consumption
of insufficiently processed bitter cassava, and a low intake of sulfur amino acids.
Method:
To determine whether an outbreak of spastic paraparesis in the Democratic Republic
of Congo was compatible with konzo, we surveyed and screened the population
in the affected area by using the WHO criteria. Interviews and focus group discussions
were done on diet and the occurrence of konzo. Serum samples were analyzed for
prealbumin, albumin and thiocyanate; urine samples for linamarin, thiocyanate
and sulfate. Serum samples were tested for HIV 1-2 (Behring ELISA) and HTLV
I-II antibodies (ELISA/Wellcome).
Results:
Of 2,723 inhabitants, 55 were affected by konzo i.e. a prevalence of 20 per thousand.
The main symptom was a sudden onset of a non-progressive spastic paraparesis or
a tetraparesis in severe cases. Bitter cassava was the staple diet. We found high
exposure to cyanogenic compounds i.e., mean (± SD) concentration of serum
thiocyanate 502 (±153) mmol/L, of urinary linamarin
482 (±322) mmol/L, and urinary thiocyanate 1128
(±670) mmol/L. The mean (± SD) urinary sulfate
concentration was 4.0 ± 3.3 mmol/L. Most subjects had low proteins concentration
in serum: of 38 subjects 37 and 28 were below the albumin and prealbumin reference
values respectively. All 38 blood samples were negative to the tested retroviruses.
Conclusion:
This outbreak was compatible with konzo. Improving cassava processing might
prevent the disease.
Key words: acute spastic
paraparesis, , cassava, cyanogens exposure, konzo.
RÉSUMÉ
Description:
Le Konzo est une paraparésie spastique permanente, à début
brutal, associée à la consommation de manioc insuffisamment traité
avec une alimentation pauvre en acides aminés soufrés.
Objectif:
Déterminer si une épidémie de paraparésie spastique
en République Démocratique du Congo était compatible avec
le konzo.
Methode:
Un dépistage des cas de konzo a été effectué au
moyen des critères de l' OMS. Des interviews ont été réalisées
sur l'alimentation et la maladie. Les taux sériques de préalbumine,
albumine et thiocyanate furent mesurés ainsi que ceux de linamarine,
thiocyanate et sulfate dans les urines. Les serums furent testés pour
HIV 1-2 (Behring ELISA) et HTLV I-II (ELISA/Wellcome).
Resultats:
Sur 2.723 habitants, 55 étaient affectés par le konzo, soit une
prévalence de 20 pour mille. Le symptôme majeur était une
paraparésie spastique permanente à début brutal ou une tétraparésie
dans les cas sévères, le manioc amer était l' aliment de
base. Il y avait une importante exposition aux substances cyanogénétiques:
concentration moyenne (± écart-type) de thiocyanate sérique
502 (±153) mmol/L, de linamarine urinaire 482
(±322) mmol/L, de thiocyanate urinaire 1128 (±670)
mmol/L. La concentration moyenne (± écart-type)
de sulfate urinaire était 4.0 ± 3.3 mmol/L. En majorité, le
taux des protéines sériques était en dessous de la normale:
sur 38 sujets, 37 et 28 l'avait pour l'albumine et la préalbumine respectivement.
Tous les 38 serums collectés étaient négatifs aux rétrovirus
testés.
Conclusion:
Cette épidémie était compatible avec le konzo. Ameliorer
le traitement du manioc peut prevenir la maladie.
Mots
clés: manioc, konzo, paraparésie spastique aigue, substances
cyanogènes.
INTRODUCTION
Spastic paraparesis has been documented both in local outbreaks and in endemic
areas in different geographical areas of the world. Various factors have been
associated with these epidemics or endemics; for instance, the retrovirus Human
T-Lymphotropic Virus, type I (HTLV - I) in HTLV-I-associated myelopathy (HAM)(1,47),
the over-consumption, with a restrictive diet, of the grass-pea (Lathyrus Sativus)
in lathyrism (5,12) and the consumption of insufficiently processed bitter cassava
with a low intake of sulfur amino acids in konzo (11). A syndrome called tropical
ataxic neuropathy (TAN) has also been associated with the consumption of insufficiently
processed bitter cassava, though it has been clinically connected with predominantly
sensory disturbances(10).
In 1996, we made a neuroepidemiological study of an outbreak of a spastic
paraparesis, suspect of konzo, in Bandundu province of the Democratic republic
of Congo (DRC). The aim of the study was to determine if this outbreak was
compatible with konzo, and to investigate if the disease was associated to the
same possible causal factors as in previous studies in other parts of
Africa.
MATERIAL AND METHODS
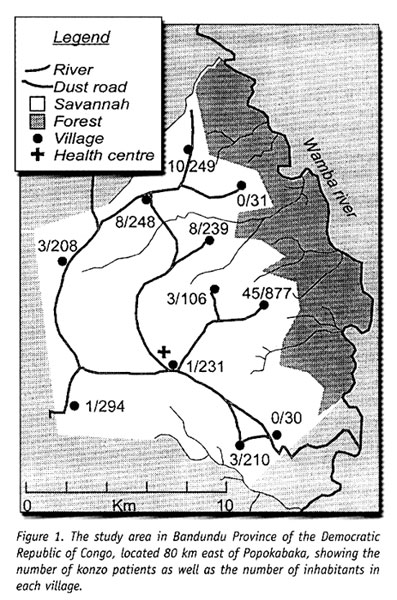
Study area
Bandundu Province, in the Democratic Republic of Congo, is situated southeast
of the capital Kinshasa (2°-8° south and 16°-20°
east). It covers 295,000 km2 with a population of 3.7 million in
1984, according to national demographic statistics (6). Popokabaka Health Zone
is located in the southwestern part of this province. It consists of a savanna
tableland with poor sandy soils intersected by forested, relatively more fertile
river valleys running in roughly south - north. The population lives mainly
in villages, growing cassava as their major subsistence and cash crop. Due to
a reported high prevalence of the disease at Masina Health Center, we selected
the Masina catchment area (14 x 14 km), situated 90 km east of Popokabaka township
as the study area (Fig.1).
Methods
The study was done in August 1996. With informed consent and assistance from
village leaders, a demographic census was performed in all 11 villages in the
area. The inhabitants were registered according to ethnic affiliation, sex, and
age group (children <15 years, adults ≥15 years). The population in
each village was screened for konzo by examining all persons with walking
difficulties identified by village leaders or health staff. The WHO criteria
for konzo (15) were applied: a visible symmetric spastic abnormality when
walking and/or running, a history of abrupt onset (< 1 week), a
non-progressive course, in a formerly healthy person, showing bilaterally
exaggerated knee and/or ankle jerks without signs of spinal disease. Those
fulfilling the criteria for konzo were interviewed in Kiyaka, the local
language, according to a standardized questionnaire regarding the time of onset
and the diet at onset. Information on year of onset was cross-checked with dates
on birth certificates available for neighboring children. Month of onset was
determined by use of a local event calendar. Thereafter, konzo-affected persons
were invited for a detailed neurological examination by a neurologist (D.T.)
including evaluation of higher cerebral functions, as well as an evaluation of
the cranial nerve function, and of motor, sensory, autonomic and cerebellar
functions. The severity of the disease was graded according to the WHO
classification (15) (mild form = walking without support, moderate form = using
one or two sticks, severe form = unable to walk). Other clinical signs were
recorded and the size of the thyroid gland assessed according to the new WHO
classification (16): grade 0 = no goiter, grade 1 = palpable goiter, grade 2 =
visible goiter. Konzo subjects who had died were traced and characterized
through interviews with the nurse at the Health Center, relatives and
neighbors. Focus group interviews (3) with 5-9 adult participants of mixed
ages were performed in the nine largest villages. A set of open questions was
introduced concerning the village, seasonal and annual variations in
agriculture, cassava processing, cassava marketing, diet, and konzo, a
well-known disease in the area. A new semi-quantitative field assay for
urinary thiocyanate was developed and used to screen 20-30 urine samples in each
village, for thiocyanate content. This new method is a modification of the
previous thiocyanate method (8) suitable for field surveys and yielding
immediate semi-quantitative results. It distinguishes ordinary concentrations
(below 100 µmol/L) from elevated levels (above 300 µmol/L). A
blood specimen and spot urine samples were collected from examined konzo
patients. Specimens were analyzed at the Department of Clinical Chemistry at
Uppsala University Hospital in Sweden. Serum was analyzed for prealbumin,
albumin, C-Reactive Protein, creatinine and thiocyanate (8). Urine was analyzed
for linamarin (2), thiocyanate (8) and sulfate (9). Serum and urinary
thiocyanate and urinary linamarin served as indicators of cyanogen exposure,
whereas albumin, prealbumin, and sulfate served as protein status
indicators. Virological tests for HIV 1-2 (Behring ELISA) and HTLV I-II
antibodies (ELISA/Wellcome) were carried out at the Department of Microbiology,
Uppsala University Hospital.
RESULTS
The Masina Health Center catchment area consists of 11 villages with, in august
1996 a total of 490 households and 2,723 inhabitants (551 men, 755 women, 714
boys <15 years and 703 girls <15 years), giving a mean of 5.5 persons
per household. The number of inhabitants in each of the 11 villages is given
in Fig.1. Yaka was the only ethnic group
in the area.
Occurrence of konzo
Of 152 persons with walking difficulties, 55 fulfilled the criteria of konzo,
thus a prevalence of 20 per thousand inhabitants in the study area. The remainder
(97/152) had disabilities of various other origins: pain in the joints of lower
limbs (92), psychosomatic disorder (2), possible disk hernia (1), myositis (1),
and foot injury (1). A typical history of konzo was also obtained for another
27 named persons, 12 of whom had moved to neighboring villages outside the catchment
area or to the capital, Kinshasa. Two of these were visited in their homes in
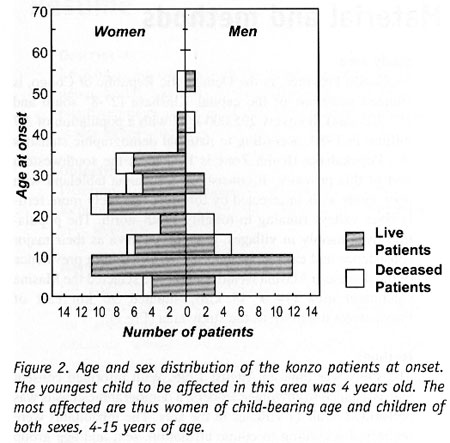
Kinshasa for interview and examination. The other 15 were deceased. Of the 82
persons thus identified as being affected by konzo, 20 were boys below 15 years
of age at the time of onset, 23 were girls, 7 men aged 15 years or more, and
32 women aged 15 years or more. The age and sex distributions are presented
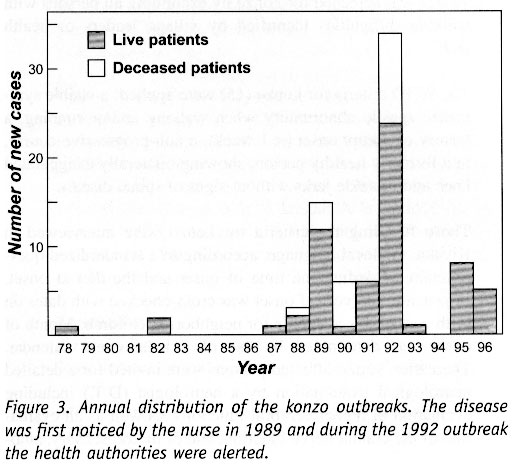
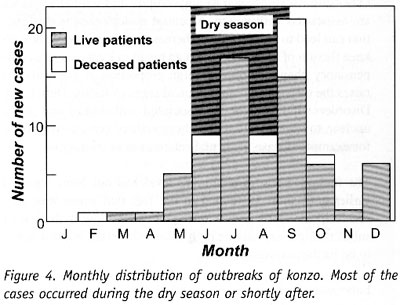
in Fig. 2. The annual and monthly distributions
of the onset of konzo are shown in Fig. 3
and 4, respectively.
Clinical findings
Symptoms at onset of konzo All patients (57) were formerly healthy
subjects who had experienced a sudden onset of gait difficulties, often preceded
by prolonged physical exercise; for instance 25 of the patients (44%) had been
walking from the forest to the village. Apart from the walking difficulties,
other symptoms were reported, such as trembling of the lower limbs by 29 persons
(51%), pain in the legs in 27 (47%) and paresthesia of the legs in 12 (21%).
Furthermore, 9 patients (16%) experienced blurred vision, 5 (9%) muscle cramps
and 3 (5%) a sensation of electrical discharges in the lower limbs at the time
of the onset. Evolution and severity of the disease The mean
duration of the disease, from the onset to the initiation of this study, was 4
years 8 months, ranging from 1 month up to 8 years, except in one subject who
had contracted the disease 18 years earlier. Most subjects (45/57, 79%)
reported a stable clinical course of the disability since the onset. Seven
subjects (12%) reported a functional improvement, whereas 5 (9%) reported one or
two abrupt aggravations during the course of the disease. Two patients (4%) had
moved to the capital Kinshasa since disease onset, respectively 2 and 7 years
before the study period. In spite of this, they still reported an unchanged
clinical course at the interview. Regarding the severity of the disease, 38
subjects (67%) had a mild form, 12 (21%) a moderate and 7 (12%) a severe form.
Neurological signs Forty subjects (70%) had the typical spastic
gait with knee flexion and "toe walking"; the spasticity increased
in the lower limbs when walking. Nine subjects (16%) walked with hyperextended
knees and on the soles of their feet, thus counteracting (and masking) a
tendency to toe walk. Seven subjects (12%) were unable to walk at all. One had
spasticity only when running.
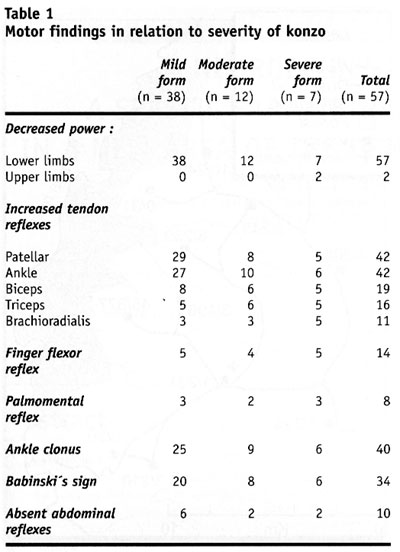
Table 1. shows the motor findings in
relation to the severity of konzo. All subjects had decreased muscle power in
the extensors of the lower limbs. Two of the seven subjects severely affected
by konzo had tetraparesis. Tendon reflexes were exaggerated in the lower limbs
in 42 patients (74%), while in the remainder the reflexes were difficult to
elicit due to joint contractures or ankylosis. Ankle clonus was found in 40
cases (70%) and was similarly difficult to elicit in the remainder. Babinski's
sign was found in 34 subjects (60%) and no response in the remainder. All patients
except 6 (11%) with joint contractures, had symmetric clinical signs in their
limbs. Ten subjects (18%) lacked cutaneous abdominal reflexes. Eight subjects
(14%) presented a bilateral palmomental reflex.
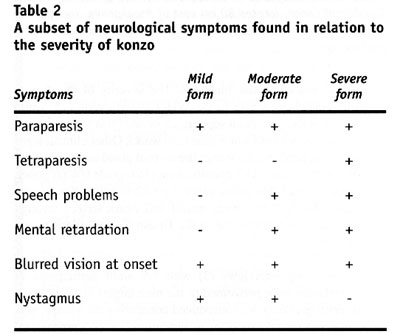
Table 2
Speech problems of
dysarthric type were found in 14/57 patients (25%) with either the moderate or
severe form of konzo. Thirteen subjects (23%) with either mild, moderate, or
severe konzo reported impaired visual acuity at the onset of the disease.
Rotatory nystagmus was observed in 3 subjects (5%) with onset at 2, 8 and 12
years of age, having a mild or moderate form of konzo. One 11-year-old subject
showed mental and physical retardation and had spastic tetraplegia with
bilateral palmomental reflex and Babinski's sign. He had contracted the
disease 4 years earlier, in its mild form, but had two abrupt aggravations, one
3 years after the onset and the other 6 months before the study. Subsequently
and simultaneously he lost the ability to walk, to speak and to swallow. He was
still unable to walk at the time of the study. No cerebellar dysfunction
was found in the patients. Sensory disturbances (touch, pain, position, and
vibration) or autonomic symptoms (such as disturbance of urethra - and/or
anal sphincter and sexual functions) were not found or reported, except for
paresthesia and the sensation of electrical discharges in the lower limbs at
onset. Other clinical signs Distal amyotrophy in arms and/or legs
was found in 4 subjects (7%), and lumbar kyphosis in 3 cases (5%). Thirty-six
patients (63%) had goiter; of these 27 (47%) had grade 1 goiter and 9 (16%)
grade 2. Various signs of malnutrition (discolored hair, skin desquamation,
edema) were found in 7 cases (12%).
The diet
The focus groups revealed that people relied on bitter cassava as their
staple diet. Shortcuts in the processing of cassava roots are common -
e.g. usually only 2 nights of soaking. Especially since 1992, shortcuts in
processing had become common as a result of the intensive trade in cassava to
Kinshasa. All the konzo patients ate the traditional cassava-flour based dough
every day as staple. Cassava leaves were the most commonly eaten supplementary
food. Meat and fish were not yet eaten daily in the villages. Lathyrus
Sativus was not known at all or seen in the area.
Laboratory findings
Urinary thiocyanate testing by the semi-quantitative method in 213 randomly
selected villagers in the area showed that 160 (75%) of the urine samples
contained thiocyanate more than 300 µmol/L.
In the 51/57 urine samples obtained from the konzo patients, the mean (±SD)
concentration of linamarin was 482 (±322) mmol/L, of thiocyanate 1128
(±670) mmol/L, and of sulfate 4.0 (±3.3)
mmol/L.
Of the 38 blood samples, all proved
negative to all four tested retroviruses (HIV-1, HIV-2, HTLV-I and HTLV-II).
C-Reactive Protein was normal in all except one who had a slight increase (21
mg/L). The mean concentration of albumin was 28 (±5) g/L, all except one
below the reference value of 40-52 g/L; of prealbumin 0.2 (±0.05) g/L, 28
of 38 patients being below the reference value of 0.225 g/L. The mean (±SD)
concentration of thiocyanate was 502 (±153) mmol/L. Serum creatinine
was clearly elevated (>100 mmol/L) in 21 of the 38 subjects, the range
being 42 - 280 mmol/L. DISCUSSION This outbreak
shared many characteristics with those previously described in Bandundu. Age and
sex distributions and the seasonal variation are similar to those in earlier
reports (11). The interview findings also confirm that the population in this
area is using short-processed bitter cassava and that this short-processing has
become more common as a consequence of intensified trade in cassava to Kinshasa.
The high concentrations of thiocyanate in the urine of the general population
confirm that the consumption of short-processed cassava exposes the people to
dietary cyanogens. The main clinical sign of konzo is a spastic
paraparesis, as previously described in several studies(11). The disease has a
sudden onset, starting mainly with trembling in the legs. The handicap remains
irreversible and may be exacerbated by further attacks, leading to severe
disability. The disease is sometimes associated with other symptoms related to
cranial nerve involvement (visual impairment) and/or pseudobulbar signs (speech
or swallowing difficulties). Most subjects show a symmetrical clinical picture,
except when joint contractures or ankylosis are present. The proportion of
neurological signs increases with the severity of konzo. This involves mainly
the addition of abnormalities in the upper limbs (increased tendon reflexes and
/or decreased muscle power), leading to tetraplegia in severe cases. In this
respect konzo shares similarities with the spastic diplegia of cerebral
palsy. The nystagmus found in 3 subjects (5%) with onset at 2, 8, and 12
years of age raises the question whether it should be considered a sign of
konzo. This symptom might be of clinical importance, since it has also been
described in 2 patients with konzo in the Central African Republic (14). The
palmomental reflex has not been reported in previous studies. Although it might
support brain dysfunction, it is known that it can occur in healthy subjects in
the general population. The mental retardation, found in one patient, raises the
question whether konzo also affects mental capacity. Indeed, this subject lost
his mental faculties as soon as he experienced two further attacks of konzo,
which exacerbated his motor disability. On the other hand, this patient might
have had an initial encephalopathy, and konzo could have impaired his condition
further, or vice versa. Other clinical signs such as amyotrophy and lumbar
kyphosis are associated with konzo. A central motor neurone dysfunction can lead
to amyotrophy, whereas the typical toe-walk with knee flexion of konzo subjects
can result in kyphosis as a compensatory phenomenon. The high proportion of
goiter (63%) raises the question whether clinical signs of Iodine Deficiency
Disorders (IDD) might be associated with konzo and make unclear, to some extent,
the pathogenesis of certain symptoms, for example in case of mental retardation
or nystagmus. The increased serum creatinine level has not been reported
earlier and could be related to the fact that water was very scarce in the study
area. Consequently, the low hydration of subjects might explain the high values
observed, but this needs to be further evaluated. Laboratory findings
demonstrated high cyanogens exposure in connection with low protein intake and
the absence of retroviruses antibodies, as found in previous konzo study areas
(11,13). Cyanogenic glucosides and their metabolites are therefore once again
linked to konzo.
ACKNOWLEDGEMENTS
We are grateful to the population of
the Masina Health Center catchment area, the local authorities, the Catholic
sisters at Imbela Mission, Kidiya Mwamba, nurse in charge of the Masina Health
Center, and Dr Gaspard Matumina at Popokabaka General Hospital for their prompt
alerting of the konzo outbreak. We also thank Professor Jonas Blomberg,
Department of Medical Sciences, Virology, for undertaking the virological tests.
We are also grateful to Lena Carlsson, Department of Clinical Chemistry at
Uppsala University Hospital, for the idea, the elaboration and the testing of
the thiocyanate field method. This study was supported by SAREC, the Swedish
Agency for Research Cooperation with developing countries and the International
Science Programme at Uppsala University, Sweden.
REFERENCES
- BHIGJEE AI, WILEY CA, WACHSMAN W, AMENOMORI T, PIRIE D, BILL PL, ET AL.
HTLV-I-associated myelopathy: clinicopathologic correlation with localization
of provirus to spinal cord. Neurology 1991; 41:1990-2.
- CARLSSON L, MLINGI N, RONQUIST G, ROSLING H. A specific and sensitive method
for the determination of linamarin in urine. Natural Toxins 1995; 3: 378-382.
- DAWSON S, MANDERSON L, TALLO V. The focus group manual. Geneva: UNDP/World
Bank/ WHO; 1992.
- GESSAIN A, GOUT O. Chronic myelopathy associated with human T-lymphotropic
virus type I (HTLV-I). Annals of Internal Medicine 1992;117: 933-946.
- HAIMANOT R, KIDANE Y, WUHIB E, KALISSA A, ALEMU T, ZEIN Z, ET AL. Lathyrism
in rural northwestern Ethiopia: a highly prevalent neurotoxic disorder. Int
J Epidemiol 1990;19: 664-672.
- INSTITUT NATIONAL DE LA STATISTIQUE RéPUBLIQUE DU ZAïRE. Résultats
provisoires du recencement scientifique de la population du 1er juillet 1984:
Institut National de la Statistique, République du Zaïre; 1984.
- KAYEMBE K, GOUBAU P, DESMYTER J, VLIETINCK R, CARTON H. A cluster of HTLV-1
associated tropical spastic paraparesis in Equateur (Zaire): ethnic and familial
distribution. J Neurol Neurosurg Psychiatry 1990; 53: 4-10.
- LUNDQUIST P, KAGEDAL B, NILSSON L. An improved method for determination
of thiocyanate in plasma and urine. Eur J Clin Chem Clin Biochem 1995; 33:
343-349.
- LUNDQUIST P, MåRTENSSON J, SöRBO B, ÖHMAN S. Turbidimetry
of inorganic sulfate, ester sulfate, and total sulfur in urine. Clinical Chemistry
1980; 26: 1178-1181.
- OLOWULE O, ONABOLU A, LINK H, ROSLING H. Persistence of tropical ataxic
neuropathy in a Nigerian community. J Neurol Neurosurg Psychiatry 2000; 69:
96-101.
- ROSLING H, TYLLESKäR T. Neurotoxicological effects of cassava cyanogenesis.
In: Spencer PS, Schaumburg H, editors. Experimental and clinical neurotoxicology.
New York: Oxford University Press; 1999. p. 338-43.
- SPENCER P, ROY D, LUDOLPH A, HUGON J, DWIVEDI M, SCHAUMBURG H. Lathyrism:
evidence for role of the neuroexcitatory aminoacid BOAA. Lancet 1986; ii:1066-1067.
- TYLLESKäR T, BANEA M, BöTTIGER B, BIBERFELD G, ROSLING H. Konzo,
an epidemic spastic paraparesis in Africa, is not associated with antibodies
to HTLV-I, HIV or HIV gag-encoded proteins. Journal of Acquired Immune Deficiency
Syndromes and Human Retrovirology 1996; 12: 317.
- TYLLESKäR T, LéGUé F, PETERSON S, KPIZINGUI E, STECKER
P. Konzo in the Central African Republic. Neurology 1994; 44: 959-961.
- WHO. Konzo, a distinct type of upper motoneuron disease. Wkly Epidemiol
Rec 1996; 71: 225-232.
- WHO/UNICEF/ICCIDD. Indicators for assessing iodine deficiency disorders
and their control programmes. WHO/UNICEF/ICCIDD; 1992. Report No.: NUT/94.6.
Copyright 2001 - African Journal of Neurological Sciences
The following images related to this document are available:
Photo images
[ns01003f3.jpg]
[ns01003f4.jpg]
[ns01003t2.jpg]
[ns01003f1.jpg]
[ns01003t1.jpg]
[ns01003f2.jpg]
| 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}