
|
African Journal of Neurological Sciences
Pan African Association of Neurological Sciences
ISSN: 1015-8618
Vol. 20, Num. 1, 2001, pp. 21-26
|
African Journal of Neurological Sciences, Vol. 20, No. 1, 2001, pp. 21-26
ACCURACY OF THE SIRIRAJ STROKE SCORE IN DIFFERENTIATING CEREBRAL
HAEMORRAGHE AND INFARCTION IN AFRICAN NIGERIANS
Abayomi S OGUN , Stephen OA OLUWOLE*, Oluremi AOGUNSEYINDE**, Abiodun O FATADE***,
Franck OJINI****, FI, Kayode A ODUSOTE*****.
Department and Institutions: Dept. of Medicine; Ogun State, University Teaching
Hospital Sagamu.
* Dept. of Medicine, UCH; Ibadan.
** Dept. of Radiodiagnosis, UCH; Ibadan.
* ** Radmed diagnostic centre; Lagos.
**** Dept. of Medicine, LUTH, Lagos.
***** West African Postgraduate Medical College, Lagos.
Correspondence/ Request for reprints : S.A. Ogun, Dept of Medicine, Ogun State
University, Teaching Hospital; Sagamu., Ogun State. Nigeria. yomiogun@skannet.com.ng
Code Number: ns01006
ABSTRACT
Background:
Scoring systems based on discriminant analysis technique and multivariate logistic
regression have been developed to distinguish cerebral haemorrhage (CH) from
cerebral infarction (CI). This distinction is necessary in the acute management
of stroke patients. The Siriraj stroke score (SSS) was evaluated in Siriraj
hospital, Bangkok, and the Western Infirmary, Glasgow, and needs to be validated
in an African setting.
Methodology:
The computerised tomography (CT) brain scans of all patients referred with clinical
diagnosis of stroke at the University College Hospital (UCH), Ibadan, and RADMED
diagnostic centre, Lagos were retrieved and reviewed as well as the case notes
of the patients at the referral hospitals. The SSS was computed and the stroke
subtype classified. This was compared with the CT scan diagnosis using the latter
as the gold standard. Data analysis was performed with Epi-info software and
by standard statistical methods.
Results:
Ninety-six patients had complete clinical records and CT scan features consistent
with stroke. Of these, 52 had cerebral infarction (CI) and 44 had cerebral haemorrhage
(CH). SSS had sensitivity of 50% for CH and 58% for CI with an accuracy of 54.2%.
Conclusion:
In this study, the SSS was not sufficiently sensitive to differentiate between
CH and CI in Africans. A prospective study with larger sample size and modification
of the discriminant variables is suggested. For now, while efforts must continue
to find a simple clinical scoring system to differentiate between CH and CI,
we contend that CT scan should remain the investigative technique of choice
and should be made affordable and available.
Keywords : Africa, cerebral haemorrhage cerebral infarction,Nigeria,
stroke, CT-scan.
RÉSUMÉ
Introduction :
Dans le but d'agir avec efficacité dans la prise en charge thérapeutique
des accidents vasculaires cérébraux un score discriminant à
l'aide de variables multiples a été élaboré afin
de distinguer les accidents vasculaires hémorragiques (AVCH) des accidents
vasculaires ischémiques (AVCI). Le Siriraj stroke score (SSS) a été
évalué au Siriraj hospital, Bangkok et au Western infirmary, Glasgow.
Il importait de le valider dans le cadre africain.
Methodologie :
Les dossiers des malades hospitalisés au Centre Hospitalier Universitaire
d'Ibadan et au centre diagnostic RADMED à Lagos ont été
étudiés rétrospectvement de même que les CT-scan.
Les données scannographiques ont été comparées au
SSS. Les informations ont été analysées grâce au
logiciel Epi-info et à l'aide de différentes méthodes stastistiques.
Résultats :
96 patitents ont été retenus. 52 malades avaient un infarcissement
cérébral et 44 une hémorragie cérébrale.
Le SSS avait une sensiblité de 50% pour les AVC hémorragiques
et 58% pour les AVCI avec une spécificité de 54,2%
Conclusions :
Cette étude permet de conclure en l'absence de spécificité
du SSS dans la distinction des AVCH et AVCI chez les Africains. Une étude
prospective est préconisée en modifiant certaines variables. Actuellement
le CT-scan reste la technique de choix pour différencier les AVCI des
AVCH.
Mots-clés:
Accident vasculaire cérébral hemorragique, Accident vasculaire
cérébral ischémique, Afrique, Nigeria, tomodensitométrie.
INTRODUCTION
Stroke is a common neurological problem accounting for a third of all
deaths in western countries [25] and about 4.5% to 17% of all deaths [2,14] and
2.3% to 8.7% of all admissions [14,16] in hospital based studies in Nigeria. The
majority of acute stroke is caused by cerebral infarction [12,16], although,
there was a suggestion of an increase in the proportion of haemorrhagic stroke
in our population [15]. Accurate and prompt clinical diagnosis is
crucial in patients presenting with sudden onset focal neurological deficits.
Hence it is important for clinicians to be able to distinguish between cerebral
haemorrhage (CH) and cerebral infarction (CI) in cases of acute stroke, since
clinical management of the two disorders differs substantially [5]. The
diagnosis of stroke is largely clinical in most developing countries as very few
centres have facilities for brain imaging. The clinical accuracy of distinction
of stroke from non-stroke has a sensitivity of up to 95% (5,18] and specificity
between 66 to 97% (9,10). However, this accuracy drops significantly when stroke
subtypes have to be distinguished, with sensitivity of 68% and specificity of
67% [4,11,23]. Despite its limitations, Computerised Tomography (CT) scan
has greatly improved the accuracy and precision of the diagnosis of stroke and
its subtypes [9,14]. It has been recommended for all patients with clinical
features of stroke because all subsequent therapeutic decisions depend on its
result [1,23]. However, CT is not readily available in most centres in
sub-Saharan Africa, where distance and cost limit access. Hence, most patients
with stroke are treated without the benefit of a CT scan and they risk being
inappropriately treated. Scoring systems based on discriminant analysis
technique have been developed, such as the Guy's hospital score [3] (also
known as the Allen score) and the Siriraj Stroke Score (SSS) [17]. Clinical
scores were also designed by multivariate logistic regression (6). These are
simple, cheap and practical means of distinguishing CH from CI but are not
sufficiently sensitive to replace CT scan. The scores were each developed on one
group of patients in a single location and therefore need to be validated in as
many other patient groups as possible. The Guy's hospital score has been
evaluated with data from the Oxfordshire community stroke project (OCSP) [10]
and at the National Hospital for Nervous Diseases, London [19]. The Siriraj
stroke score has been evaluated [17] in Siriraj hospital, Bangkok, Thailand and
also at the Western infirmary, Glasgow [24]. The clinical score by Besson was
also validated in the University Hospital of Grenoble, France [6]. None of them
has been evaluated in an African population to the best of our knowledge.
This study aimed to determine the sensitivity, specificity and accuracy of
Siriraj scoring system in distinguishing between CH and CI in stroke patients
confirmed by CT scan.
METHODOLOGY
Records of computerised tomography (CT) of the brain done between 1991
- 1999 at University College Hospital (UCH), Ibadan, and RADMED diagnostic
centre, Lagos were reviewed. The CT brain scans of all patients referred with
clinical diagnosis of stroke were retrieved and reviewed by two of the authors
(A.O.,B.F). The case notes of these patients at the referral hospitals were also
retrieved and reviewed by the neurologists (S.O.,O.O.,F.O) in the team. A
questionnaire was designed to extract relevant clinical data from the case
records. The questionnaire recorded the age, sex, date of admission and
discharge from hospital, presence of headache, vomiting, loss of consciousness,
the level of blood pressure, history of hypertension, transient ischaemic
attacks, diabetes mellitus, obesity, angina pectoris, intermittent claudication,
haemoglobinopathy, atrial fibrillation and cholesterol level. The stroke type
and anatomic localisation were also recorded. Some patients were comatose on
admission and the history was obtained from relations. Only patients with
adequate clinical notes were included in the study. The Siriraj stroke score
was calculated as (2.5 x level of consciousness) + (2 x vomiting) + (2 x
headache) + (0.1 x diastolic blood pressure) - (3 x atheroma markers)
- 12. A score above +1 indicates intracerebral haemorrhage, while a score
below - 1 indicates infarction. A score between - 1 and +1 represents
an equivocal result needing a CT scan to verify the diagnosis. (Appendix 1)
The SSS was computed for each patient, and based on the individual score,
the patients were classified into CH or CI using the criteria > +1 for CH and
< -1 for CI [17]. Patients with scores between +1 and - 1 were
unclassified. The classification of the stroke subtypes using SSS was compared
with the CT scan diagnosis, which was taken as the gold standard. The CT
of the brain was done with G.E. CT. MAX 640 in Lagos and G.E. 9000 in Ibadan,
using 5mm slices at 5mm intervals at the base of the skull and 10mm slices at
10mm intervals for the rest of the brain. Contrast enhancement was performed
only in patients with atypical hypodense lesions. The interval between the time
of the culpable ictus and the CT scan was recorded and ranged from 5 to 15 days
with a mean of 10 + 0.6 days.
Data analysis for sensitivity, specificity, accuracy, frequency distribution,
histogram, receiver-operating characteristic curve and cut-off determination
of the scores were performed with the Epi-info software and by standard statistical
methods [20].
RESULTS
The brain CT scans of 182 patients referred
with clinical diagnosis of stroke were reviewed, 93 from University College
Hospital (UCH) and 89 from Radmed. Of these, only 96 patients (53%) had complete
clinical records and CT scan features consistent with the diagnosis of stroke,
and these formed the subjects of this study. Of the remaining 86 patients, 59
(32%) had non-stroke lesions and 21 (12%) had incomplete clinical records. The
case notes of six (3%) of the patients could not be retrieved at the referral
centre. Of the 96 patients with stroke and complete clinical records, 67
were males and 29 were females. The male: female ratio was 2.4:1. The age of the
patients ranged from 51 to 69 years with a mean of 60 + 4.3 years. Eleven
patients (12%) were comatose on presentation and history from the relations was
relied upon. Fifty-two patients (54.2%) had CT scan features of CI, whilst 44
patients (45.8%) had features consistent with the diagnosis of CH. Using the
Siriraj Stroke Score, 88 patients (91.7%) were classified, 48 (50%) as CI and 40
(41.7%) as CH. Eight patients (8.3%) had indeterminate scores.
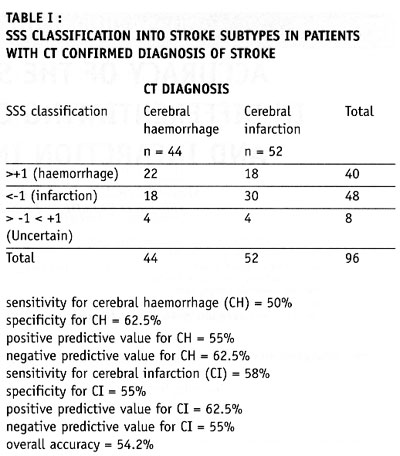
Of the 52 patients with CT scan diagnosis of CI, 30 (58%) were correctly classified
as cerebral infarction and 18 (35%) as cerebral haemorrhage using the SSS (table
I). Four patients could not be classified. Of the 44 patients with CT scan
features of CH, 22 (50%) were correctly classified as cerebral haemorrhage and
18 (41%) as cerebral infarction using the SSS. Classification was uncertain
in 4 patients (Table I). Thus, SSS had
sensitivity of 50% for CH and 58% for CI with an accuracy of 54.2%.
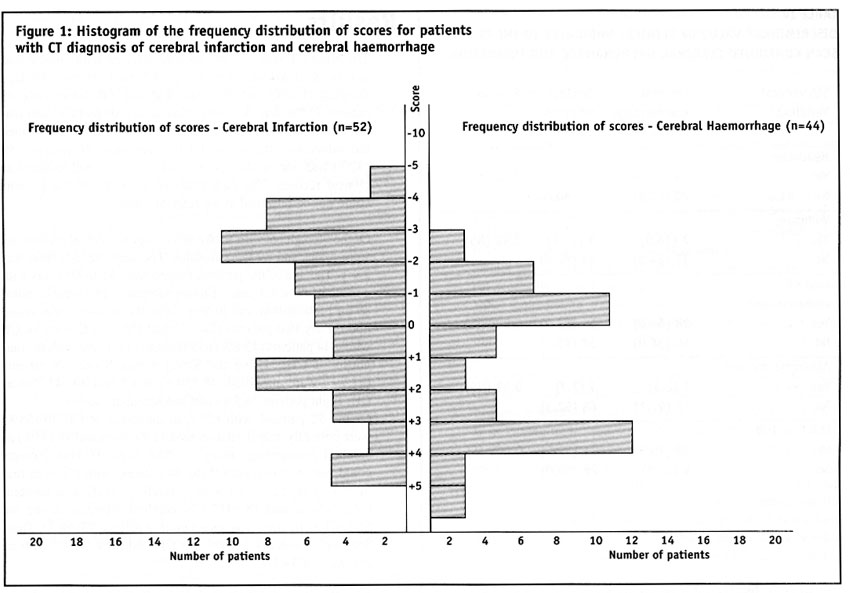
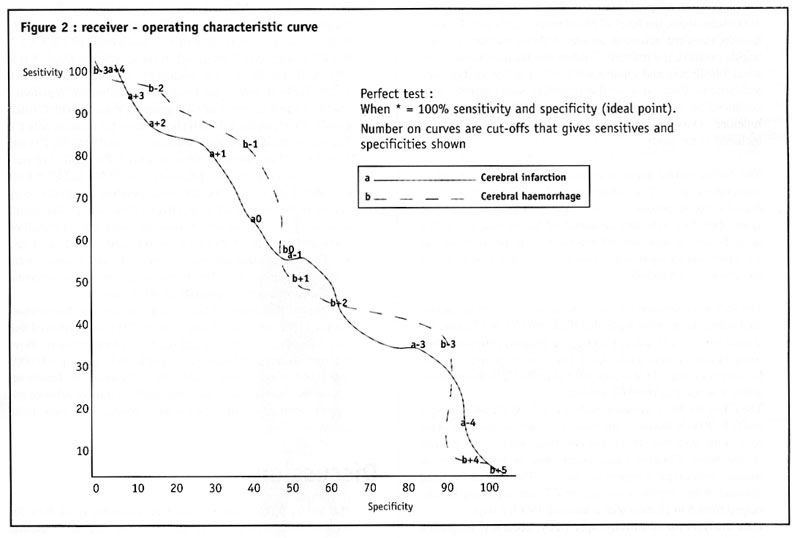
The frequency distribution of the scores of the patients grouped according
to CT diagnosis is shown in figure
1. The scores for patients with CT confirmed CH ranged from - 3.0 to +10.0,
with a mode of +3.0, median of +0.5 and a mean of + 0.8 + 2.3. For CT
confirmed CI, the range of the scores was from - 6.0 to +4.0, with a mode of
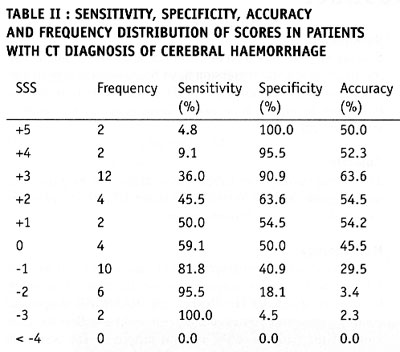
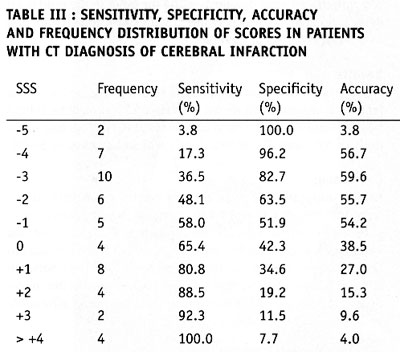
- 3.0, median of - 1.0 and a mean of - 0.9 + 2.6. Table
II shows the frequency distribution, sensitivity, specificity and accuracy
of each score for patients with CT diagnosis of CH, whilst Table
III shows those for patients with CI. The best separation or highest accuracy
was 63.6% for CH and 59.6% for CI and these occurred at scores of +3 and -3
respectively. At this cut-off, the specificity was 90.9% and 82.7% for CH and
CI respectively but the corresponding sensitivity dropped to 36.0% and 36.4%
respectively. However, at this cut-off scores, 25 (27.6%) of the 96 patients
could not be classified compared to eight (8.3%) with the standard cut-off of
- 1 and +1. Thus, no optimal sensitivity, specificity and accuracy were achieved
in this study. The Receiver-operating characteristic curve also showed no optimal
cut-off (figure 2).
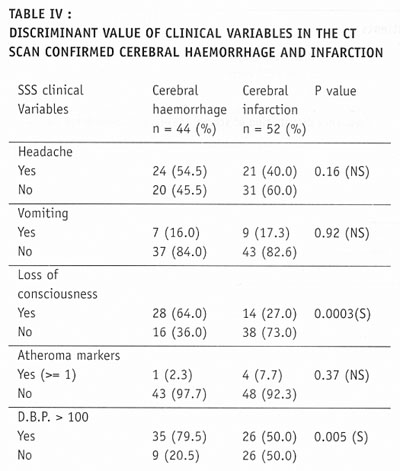
Analysis of the ability of the clinical variables to discriminate between patients
with CT diagnosis of CH and CI showed that only loss of consciousness and diastolic
blood pressure above 100 mmHg, achieved statistical significant levels of p
= 0.0003 and 0.005 respectively (Table IV).
Presence of headache, vomiting or one or more atheroma markers did not achieve
statistical significance in distinguishing between the two stroke subtypes.
DISCUSSION
The Siriraj Stroke Score (SSS) had a sensitivity of 50% for cerebral haemorrhage
(CH), and 58% for cerebral infarction (CI), with accuracy of 54.2% in this study.
This is lower than the sensitivity of 89% for CH and 93% for CI, with accuracy
of 90% reported in Bangkok, Thailand [17]. It is possible that the SSS may not
be sufficiently sensitive to differentiate between CH and CI in non-Asian population
since our findings are comparable to the study by Weir and his co-workers [24],
who showed an overall accuracy of 64% for the SSS. They had suggested its limited
use in differentiating between CH and CI in populations other than those in
Asia, and our findings appear to confirm this.
The predictive value of any diagnostic score depends greatly on the prevalence
of the disease in the area of study, and scoring systems may not be applicable
transculturally [17]. In Thailand, there is a preponderance of haemorrhagic
stroke while in the Nigerian stroke population cerebral infarction is commoner
[16]. Cerebral haemorrhage accounts for 40 - 50% of strokes in Thailand [22],
19% in Nigeria [16], 10 - 15% in Europe [6], and 20% in America [7]. Siriraj
Stroke Score appears to have high predictive values in populations with preponderance
of haemorrhagic stroke as in Asia, and low predictive values in populations
with preponderance of cerebral infarction as in Africa, Europe and America.
We were surprised that the predictive values amongst Nigerians were low despite
the recent suggestion of an increasing proportion of haemorrhagic stroke in
our population [15]. Our findings do not support the view of Celami et al. that
the use of SSS is probably better in detecting infarction than haemorrhage,
and supposedly should be applicable to Africans [8].
In this study, SSS was not sufficiently sensitive to differentiate between
CI and CH using the acceptable discriminant clinical variables and the cut-off
values. The questionable validity of accurate history in a retrospective study
could be contributory, as 12% of the patients were comatose on presentation
and reliance was placed upon history from relatives. History of headache at
the time of ictus, past history of intermittent claudication or angina pectoris
may not be obtained in such circumstances. The low occurrence of atheroma markers
such as intermittent claudication or angina pectoris in this population could
be additional factors [16]. Furthermore, the discriminant value of headache
in distinguishing between haemorrhage and infarction was low in this study (table
IV) in contrast to the findings of Besson et al. [6]. However, loss of consciousness
and diastolic blood pressure above 100, had high discriminant value in accordance
with their findings.
The best separation or highest accuracy in this study was 63.6% for
CH and 59.6% for CI at scores of +3 and -3 respectively. Our study showed that
with increasing accuracy and specificity, the diagnostic sensitivity dropped
significantly and as many as 27.6% of the patients were unclassified at the
cut-offs that gave the best separation accuracy. Although, this proportion is
comparable to the proportion of unclassified patients in the original validation
study in which 20% of their patients were unclassified [17]. The Allen score
was validated and found to have an overall predictive accuracy of 78% in Oxford
[10] and 82% in London [19]. This was however not used for this retrospective
study because it requires several historical and clinical details, and cannot be
used until 24 hours after the stroke. Also, the clinical scores by Besson [6]
had an empirical positive predictive value approaching 100%, but involve more
clinical variables than the SSS. The SSS is easier to determine and can be used
immediately after stroke. The overall predictive accuracy (64%) of Allen scores
and the SSS was similar amongst Caucasians [3], therefore, the choice of either
should depend on ease of use or other considerations. The SSS was chosen because
it involves fewer variables with the greater possibility of having more complete
data to calculate the score in this retrospective study. Moreover, it would be
easier to apply in a busy, less well-equipped clinical setting, as is prevalent
in developing countries of Africa.
Although, this study has not supported the use of the SSS in our stroke patients
using the discriminant clinical variables and the cut-off, it is unlikely that
CT scan would be widely available and easily accessible to all stroke patients
in sub-Saharan Africa in the near future. Therefore, the search must continue
for a simple clinical scoring system to differentiate between CH and CI. A prospective
study with larger sample size is suggested. Such a study may be able to determine
a more accurate cut-off point. Modification of the discriminant clinical variables
to exclude variables with low discriminant value and include variables with
higher discriminant value in the African population should be considered. Until
result of such a study is available, we contend that CT scan should remain the
only reliable investigation for distinguishing between CH and CI among African
Nigerians and it should be made available and affordable.
RFERENCES
- ADAMS HP, BROTT TA., CROSSWELL RM, FURLAN AJ, GOMEZ CR, GROTTA J.ET AL.
Guidelines for the management of patients with acute ischaemic stroke. Circulation
1994;90(3):1588 - 1601.
- ADETUYIBI A, AKINSANYA JB., ONADEKO BO. Analysis of the causes of death
on the medical wards of the University College Hospital, Ibadan over a 14
year period (1960 - 73). Trans Roy Soc Trop Med Hyg 1976;70:466 - 73.
- ALLEN CMC., Clinical diagnosis of the acute stroke syndrome. Quart. J Med
1983;208:515-523.
- ARBIN, M, BRITTON M, FAIRE U, HELMERS C, MIAH K, MURRAY V. Accuracy of
bedside diagnosis in stroke. Stroke 1981;12:288 - 293.
- BAMFORD J. Clinical examination in diagnosis and sub-classification of stroke.
Lancet 1992;339:400 - 402.
- BESSON G, ROBERT C, HOMMEL M, PERRET J. Is it clinically possible to distinguish
non-haemorrhagic infarct from haemorrhagic stroke ? Stroke 1995;26(7):1205
- 1209.
- BROWN RD JR, CSHIMANT, JP, SICKS JD. Stroke incidence, prevalence, and
survival: Secular trends in Rochester, Minnesota, through 1989. Stroke 1996;27:373-380.
- CELANI, MG, RIGHETTI, E, MIGLIACCI R, ZAMPOLINI M, ANTONIUTTI L ET AL. Comparability
and validity of two clinical scores in the early differential diagnosis of
acute stroke. B M J 1994;308:1674-6.
- EDLOW AJ, CAPLAN RL. Avoiding pitfalls in the diagnosis of sub-arachnoid
haemorrhage N.Eng J Med 2000;342:29 - 36.
- HAMFORD J, SANDERCOOK PAG, DENNIS MA. Prospective study of acute cerebrovascular
disease in the community. The Oxfordshire community stroke project 1981 -
1986: 1 Methodology, Demography and incident of first ever stroke. J Neurol.
Neurosurg. Psychiatry 1988;1373 - 80.
- HARRISON, M.J.G. Clinical distinction of cerebral haemorrhage and cerebral
infarction. Postgraduate Medical J 1980;56:629-32.
- KANNEL, WB., Wolff, PA. Epidemiology of cerebrovascular disease. In : vascular
diseases of the CNS (ed Ross Russell R.W.), London. Churchill Livingstone
1983;183-185.
- LIBMAN RB, WIRKOWSKI E, ALVIR J, RAO H. Conditions that mimic stroke in
the emergency department Arch. Neurol 1995;52:1119 - 122.
- OGUN SA, ADELOWO, OO, FAMILONI OB, JAIYESIMI AE, FAKOYA EA. Pattern and
outcome of medical admission at the Ogun State University Teaching Hospital
- A three year review.W Afr J Med 2000;19:304 - 308.
- OGUN, SA. Acute stroke mortality at Lagos University Teaching Hospital
- A five year review.Nig. Quart. J of Hosp Med 2000;10(1):5-7.
- OSUNTOKUN BO, ODEKU, E., ADELOYE RBA. Non- embolic ischaemic cerebrovascular
disease in Nigerians. J Neurol Sci 1969;9:361 - 388.
- POUNGVARIN, N, VIRIYAVEJAKUL, A, KPMONTRIC C. Siriraj stroke score and validation
study to distinguish supratentorial intracerebral haemorrhage from infarction.
B M J 1991;302:1565 - 67.
- SANDERCOCK P, MOLYNEUX A, WARLOW C. Value of CT in patients with stroke:
Oxfordshire community stroke project. B M J 1985;290:193-197.
- SANDERCOCK PAG, ALLEN CMC. CORSTON RN. Clinical diagnosis of intracranial
haemorrhage using Guy's Hospital score. BMJ 1985;291:1675 - 77. (correction
1986;292:173.)
- SIMON D, BORING JR. Sensitivity, specificity and predictive value In: Clinical
methods - 3rd edition.Ed: by H. Keneth Walker., Dallas, Hall. Hurst, W. J.
1988;pp49 - 54.
- SOTANIEMI KA, PYKTINEN J, MYLLYIA VV. Correlation of clinical and computerised
tomographic findings in stroke patients. Stroke 1990;21:1562 - 6.
- VIRIYAVEJAKUL A, POUNGVARIN N. Internal medicine patient: an analysis of
incidence, mortality rate of 27,325 admissions. Siriraj Hospital Gasette 1982;34:501-600.
- WARDLAW JM. Is routine CT in stroke unnecessary ? B M J 1994;309:1498.
- WEIR CJ, MURRAY GD, ADAMS FG, MUIR KW, GROSSET DG. Poor accuracy of stroke
scoring systems for differential clinical diagnosis of intracranial haemorrhage
and infarction. Lancet 1994;344:999-1002.
- WHITE MF. Reducing cardiovascular risk factors in the United States - an
overview of the National Educational Programs. Cardiovasc Risk Factors 1991;1:277.
Copyright 2001 - African Journal of Neurological Sciences
The following images related to this document are available:
Photo images
[ns01006t2.jpg]
[ns01006t1.jpg]
[ns01006f2.jpg]
[ns01006t4.jpg]
[ns01006f1.jpg]
[ns01006t3.jpg]
| 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}