
|
African Journal of Neurological Sciences
Pan African Association of Neurological Sciences
ISSN: 1015-8618
Vol. 21, Num. 1, 2002, pp. 26-29
|
African Journal of Neurological Sciences, Vol. 21, No. 1, 2002, pp. 26-29
INITIAL EXPERIENCE WITH STEREOTACTIC SURGERY IN WEST AFRICA
N.A.B. ANDREWS
CORRESPONDENCE to : N. A. B ANDREWS, MD, TEMA INTERNATIONAL NEUROCENTER, NARH-BITA
HOSPITAL, TEMA, GHANA, P.O.BOX B196, COMM. II, TEMA., GHANA. Email; neurogh@africaonline.com.gh, nbandrews@hotmail.com
Code Number: ns02005
SUMMARY.
BACKGROUND
The first stereotactic surgery program in West Africa was established in Ghana
in 1999.
OBJECTIVE
This study presents a retrospective evaluation of the pattern and outcome of
the first seventeen consecutive stereotactic procedures. It also discusses the
benefits, challenges and prospects of the program in West Africa.
METHODES
17 patients (11F, 6M) with CT disclosure of intracranial mass lesions that could
be assessed or managed stereotactically to the patients benefit (9,10). underwent
stereotactic procedures during a consecutive 18-month period. Analysis of charts,
relevant imaging studies and pathology reports were done.
RESULT
The average age of the patients was 37 years (range 2-72years). 71% had a preoperative
diagnosis of brain tumor; 83.3% were confirmed. All the procedures were performed
in the supratentorial compartment. A biopsy was done in every case. 35% underwent
biopsy and aspiration/evacuation. The mean CT scan time was 18 minutes (range
5-48minutes). The mean operating room time was 37 minutes (range 30-43minutes).
All the cases were done utilizing local anesthesia and intravenous sedation.
The average length of hospital stay was 2.7days (range 2-7 days). Histopathologic
results showed Arachnoid cyst (2), Neoplasms (10), infection (1), Intraaxial
hematoma (2), Thrombosis (1), Normal tissue (1). The failed biopsy rate was
6%. The surgical objectives were achieved without complications. No blood transfusions
were given or required. Stereotactic procedures cost 50-59% less than conventional
surgery.
CONCLUSION
It is concluded that the initial experience with stereotactic surgery in West
Africa consists of utilizing the Leksell Stereotactic System for the safe performance
of tumor biopsies and aspirations/evacuations with reduction in health care
costs compared to conventional surgery
KEY WORDS : Neurosurgery, Stereotactic surgery, West Africa.
RÉSUMÉ
INTRODUCTION
Les premières interventions stérotaxiques ont été
réalisées en 1999 au GHANA.
OBJECTIF
Notre étude rétrospective évalue les caractènes
cliniques,paracliniques ainsi que le traitement et l'évolution de 17
patients ayant bénéficié de ce type d'intervention
METHODES
L'étude de ces 17 patients opérés sur une péride
de 18 mois a été faite à partir des dossiers d'hospitalisation.
Le cadre de Lecksell a été utilisé.
RESULTAT
La moyenne d'âge est de 37 ans (2-72 ans). La procédure a intéressé
uniquement l'étage sus - tentoriel et a concerné tous les patients.
La durée moyenne du CT-scan a été de 18 mn et celle des
interventions 37 mn ( 30-43mn). La durée moyenne de séjour a été
de 2,7 jours (2 - 7 jours). Les lésions suivantes ont été
observées : kystes arachnoïdiens (2), néoplasmes (10), infections
(2), hématome intra axial(2), thomboses(1), tissu normal (1). Le taux
d'échec a été de 6%. Aucune complication a été
observé. Il n'y a eu aucune transfusion. La technique stéotaxique
coûte 50 à 59% moins cher que la chirurgie conventionnelle.
CONCLUSION
Cette étude préliminaire conduite en Afrique de l'Ouest permet
de conclure à l'efficacité de la stéréotaxie quant
au diagnostic, à la sécurité et aux coûts par rapport
à la chirurgie conventionnelle.
Mots clés : Afrique de l'Ouest - Neurochirurgie - Stéréotaxie,
INTRODUCTION
The introduction of CT scanners into West Africa in the last decade has upgraded
the practice of neurosurgery in the sub-region. The CT scanner provides a three
dimensional data-base of the brain. The combination of the CT scanner and stereotaxy
optimises the use of the former. Stereotactic instrumentation provides the capability
for rapid access with great accuracy to virtually any intracranial point. The
rationale for applying stereotactic methodology to neurosurgical procedures
is to access targets accurately with a minimum of spatial error (i.e. low bias)
and a high degree of reproducability (i.e. high precision ). In the management
of intracranial lesions, intracranial access can be achieved and valid answers
obtained regarding processes that required craniotomy or high risk cerebral
transit. The histological nature of any suspicious intracranial lesion may be
determined safely and accurately thereby enabling the compilation of an accurate
database for intracranial lesions. It is also possible to evacuate intracranial
hematomas; aspirate cysts or abscesses; provide guidance for small lesions;
perform functional procedures, eg for movement disorders, epilepsy and the implantation
of interstitial radioactive sources into intracranial neoplasms.
Since stereotactic surgery is a minimally invasive neurosurgical technique
that is thought to reduce hospitalization periods, blood transfusion requirements,
the need for general anesthesia and consequently health care costs, it was decided
to introduce it into Ghana; the neurosurgeon/population ratio in Ghana is 1:9million.
This study is a retrospective evaluation of the first seventeen consecutive
stereotactic procedures. It also discusses the benefits, challenges and prospects
of the program in West Africa.
MATERIALS AND METHODS.
17 patients (11F, 6M) with CT disclosure of intracranial mass lesions that
could be assessed or managed stereotactically to the patients benefit (3,4).
underwent stereotactic procedures during a consecutive 18-month period. Analysis
of charts, relevant imaging studies and pathology reports were done.
CT-Guided Stereotactic Procedure.
A Leksell G frame (Elekta AB, Sweden) was placed under local anesthesia and
CT imaging performed. Contrast material (60% meglumine iothalamate) was given
10-20 min prior to imaging. Target point selection was based on imaging morphology,
location and anticipated risk of causing complications especially hemorrhage
or neurologic deficits. The enhancing portion of a suspected tumor was usually
targeted; in a nonenhancing mass, the center of the mass was targeted. Stereotactic
coordinates were obtained using CT scanner software and verified by a manual
method.
Patients were then transported to the OR suite where under sterile conditions
and utilizing local anesthesia and IV sedation, intracranial access was obtained
via a 2mm or 4mm twist drill calvarial opening. 3-6 biopsy specimens were taken
in each case and subjected to histopathologic analysis. The safest and usually
shortest transit penetrating one pial surface was utilized while taking into
consideration the structures in the transit path to the lesion. Biopsy specimens
were obtained with a Blaklund spiral biopsy needle. Facilities for intraoperative
frozen section were not available.
No blood transfusions were required. All scalp wounds were closed with the
use of only one unit of non-absorbable suture material.
RESULTS.
17 consecutive stereotactic procedures were performed. There were 6 males and
11 females; ages ranged from 2 to 72 years with one patient under 10 years.
The mean age was 36.7 years (SD, 19.4). 16 cases (94%) achieved a definitive
diagnosis, and 1 case was classified as failed biopsy, providing a failed biopsy
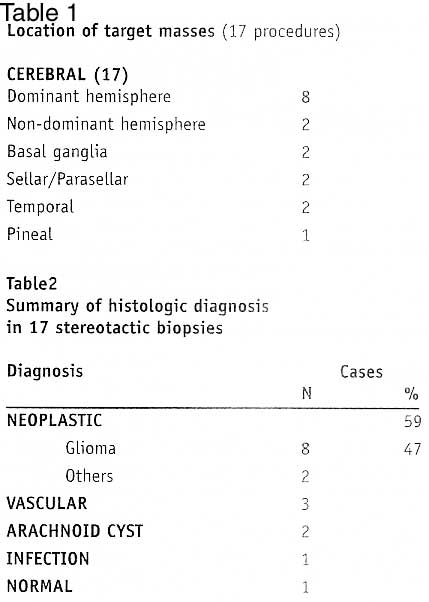
rate of 6%. The pathological findings of the overall series are presented in
table 2.
Imaging Characteristics
All the lesions were in the supratentorial compartment; there were a total
of 17 target mass lesions. There were 8 dominant hemispheric and 2 non dominant
hemispheric targets. Two targets each were temporal, sellar/parasellar, basal
ganglionic and 1 was pineal (Table
1).
In all cases, contrast-enhanced CT scans were performed in order to guide target
selection. Contrast enhancement was present in 13 of the 17 cases (76%).
The mean CT scan time was 18 minutes (R 5-48mins; SD 13).
Pathological Findings, Management.
Neoplasm constituted 59% and was the commonest histologic diagnosis 12 cases
(71%) had a preoperative diagnosis of brain tumor; 10 cases (83%) were confirmed.
80% of the neoplasms were astrocytomas and formed 47% of the entire series of
patients. Two patients had glioblastoma multiforme and 6 had low grade astrocytomas.
Two of the low grade astrocytomas had a cystic component which was aspirated.
One patient each had a pituitary adenoma and pinealoblastoma. One patient who
was thought to have an occipital glioma on biopsy turned out to have an early
bacterial abscess and cerebritis, both of which resolved completely after antibiotic
therapy.
Two patients had large ganglionic hemorrhages with mass effect and worsening
neurologic status. They both underwent stereotactic aspiration/evacuation utilizing
the Blacklund device. One died 3 days post operatively following a massive ganglionic
rebleed and a new mesencephalic hemorrhage. The other was discharged with GOS
1.
Arachnoid cysts were biopsied and aspirated in 2 patients. One of the patients
who was 2 years at the time of the procedure, had complete resolution of the
cyst confirmed by CT imaging performed 11 months after the stereotactic procedure.
She has however developed non-communicating hydrocephalus for which endoscopic
third ventriculostomy and or aqueductoplasty is planned. In total, 6 of the
cases (35%) underwent both biopsy and aspiration/evacuation.
Normal brain was retrieved in one patient. No targeting error was confirmed
by postoperative imaging. The mean duration of follow up was 9 months (R 3days-18months;
SD 6months).
Cost
The cost of stereotactic procedures was compared to the cost of conventional
craniotomy. The following parameters were used to calculate the costs of the
two kinds of procedures; 1) cost of stereotactic CT scan 2) cost of OR consumables,
viz. Anesthesia, sponges/swabs, patties, 3) laboratory tests. 4) drugs 5) cost
of 2 days stay in Intensive/Critical care unit 6) Cost of 7-10 days in hospital.
The following assumptions were made a) no stereotactic scan is required for
conventional craniotomy b) for stereotactic procedures, no days were spent in
the Intensive/Critical care unit c) 2-3 days of hospital stay is required for
stereotactic procedures as compared to 7-10 days for conventional craniotomy.
It was found using the above parameters and assumptions that stereotactic procedures
cost 50-59% less than conventional craniotomy. In the series, the average OR
time was 37 minutes (R 30-43; SD 4). The mean duration of hospital stay was
2.7 days (R 2-7days; SD 1.4).
DISCUSSION.
Two old and simple concepts, a three-dimensional positioning stage and a coordinate
system were combined in 1906 to create a new one; the stereotactic method (7).
The advent of computer-based medical imaging applied to the stereotactic method
encouraged the adaptation of the later to the management of intracranial tumors
(13). The incorporation of CT scanning into stereotactic technique in the early
1980's was an obvious step for two reasons. First, CT provided a precise 3-D
database that can be readily translated into the 3-D coordinate system of a
stereotactic frame. Second with CT scanning, tumors could be seen directly instead
of having their positions inferred from shifts of components of the ventricular
system or from shifts of vessels on cerebral angiography.
Evaluation of the enhanced anatomic detail provided by the CT scanner could
therefore be used for surgical planning. The availability of stereotactic surgical
equipment and technique therefore optimises the use of the CT scanner. Optimal
use of a CT scanner is crucial since the acquisition and maintenance of a CT
scanner involves a large capital investment. Our study reveals that the mean
CT scan time of 18 minutes required for stereotactic data acquisition can readily
be fitted into the schedule of a Radiology Department in the region without
significant disruption. Appuzo et al reported that a scan utilization time of
less than 15 minutes renders the issue of scanner access in a busy neurosurgical
service inconsequential (1). Furthermore, the acquisition of MRI equipment by
an institution in West Africa will be superfluous unless that institution has
the capability to perform stereotactic surgery.
Hitherto, localization methods for intracranial procedures in West Africa have
been qualitative and imprecise. Large skin and bone flaps have been utilized
in order to ensure that the relevant lesion lay within the limits of the craniotomy.
Consequently, general anesthesia, blood transfusions and several days of critical
post-operative care have been required. The lack of relative availability of
these resources within the sub-region has made the practice of neurosurgery
difficult and problematic. The purpose of incorporating stereotactic methodology
into neurosurgical practice is to provide an improvement in localization over
that which is available. The proper clinical use of stereotactic methodology,
requires a mature technological understanding of the available instruments and
a clear understanding of their benefits and limitations. Clinically, the determinants
of application accuracy should be considered before every use of stereotactic
methodology for any therapeutic intervention (11,18). As shown from this study,
stereotactic procedures can be accomplished without the need for general anesthesia,
blood transfusions and critical post-operative care. An added advantage is the
ability to surgically treat neurologic patients with mild or severe systemic
disease that is incapacitating or life-threatening (ASA II-IV) with much less
added risk. The average OR time of 37 minutes is much less than that required
for a conventional craniotomy.
A comparative cost analysis revealed a 50-60% reduction in total costs for
stereotactic procedures when compared to conventional craniotomy. This analysis
took into account the cost of the stereotactic CT scan, operating room costs,
pharmaceuticals and length of hospital stay. The mean duration of hospital stay
of 2.7 days is considerably lower than for conventional craniotomy. In the sub-region
almost all patients who undergo craniotomy have had to remain in hospital for
at least 7 days in order to ensure proper wound healing and suture removal before
discharge. Stereotactic procedures also reduce the need the OR swabs/sponges,
patties, scalp clips, sutures, wound drains, wound dressings and laboratory
tests. Further cost reductions are obtained by reducing the need for Intensive/Critical
care and the utilization of local anesthesia complemented by intravenous sedation
for procedures. Stereotactic procedures will help to reduce the on health care
professionals and resources in the ssub-region.
All the target lesions were in the supra-tentorial compartment. However, stereotactic
procedures can also be performed for posterior fossa lesions (1,8,12,20). Table
2 gives the histopathologic processes substantiated in the 17 biopsied lesions.
The diagnostic biopsy rate has varied between 91 and 100% (2,9). Diagnostic
success is predicated on proper case selection, precise point target tissue
retrieval and informed pathologist feedback. Proper case selection demands that
the decision to employ stereotactic biopsy should be preceeded at all times
by a thorough neurologic and radiographic assessment of the patient. Lesions
such as ischemic infarcts, vascular malformations and multiple sclerosis should
not be biopsied. The prevention of targeting error can be technically achieved
by careful data entry and the avoidance of angulation of biopsy probes at the
calvarial entry point. Real-time intraoperative imaging can in the future provide
for monitoring the biopsy needle in relation to the intended target. Finally,
the availabilty of intraoperative frozen section/smears often provides useful
information to guide the surgeon and should be used whenever possible (21).
We had to depend entirely on review of histologic sections after permanent fixation;
facilities for frozen section review are not available.
There is a wide range of failed biopsy rates in the literature, 3-47%. This
is as a result of the wide differences in definition of failed biopsy rates
(1,5,10,15,16,17,19,22,23,25,2622,24). Soo et al have classified failed biopsies
as lesional or nonlesional (24). Lesional failed biopsies reflect a nonspecific
pathologic change e.g astrogliosis, necrosis or inflammatory change. Lesional
failed biopsies can be further divided into representative and nonrepresentative.
The representative group have a time window outside which definitive diagnosis
cannot be made as the pathologic elements become less distinct e.g radionecrosis,
subacute infarction or a demylinating plaque from multiple sclerosis. In these
situations it is sometimes impossible to obtain a definitive diagnosis even
after craniotomy and open biopsy. Although these lesions are generally not biopsied,
in some instances, neither clinical judgement or current available imaging modalities
can differentiate them from neoplastic or infective processes, hence necessitating
biopsy. The lesional nonrepresentative failed biopsies are due to biopsying
either the reactive edges or the necrotic areas of hetrogenous neoplastic or
infectious processes. These may be considered as a relative target selection
error or minor targeting error. Inspite of the limited diagnostic usefulness
of lesional failed biopsy, in certain cases the pattern of the changes suggests
a specific diagnosis such as tumor necrosis versus coagulative necrosis of infarction.
In nonlesional failed biopsy, the predetermined target on a static CT scan was
missed, yielding normal brain. This may occur as a result of the lesion migrating
away from an advancing biopsy needle. A slight angular deflection of the semirigid
biopsy needle on account of an angled twist drill calvarial entry may lead to
the biopsy device missing the lesion tangentially. The failed biopsy rate for
the series is 6%. Meta-analysis of 9,467 published cases of stereotactic biopsy
from series with over 100 cases yields a failed biopsy rate of 9%.(24).
It has been commonplace to blame diagnostic failure on the size of the biopsy
specimen, i.e it is too small (14). However a representative specimen is always
of sufficient size for a diagnosis to be made and representative tissue is better
obtained with stereotactic technique than with open biopsy methods (6). The
elucidation of the molecular pathogenesis of CNS tumors will hopefully lead
to a to a molecular classification and enable improved diagnostic yields from
small stereotactic biopsy specimens, eg DNA analysis using polymerase chain
reaction requires less than 100ng of DNA to identify infectious agents such
as toxoplasma; differntiation of astrogliosis from a low grade glioma using
molecular markers such as p53 mutation, loss of genetic information on chromosome
19q or over expression of growth factor receptors implicated in tumorigenessis
(24).
From an initial start of biopsies and aspirations/evacuations, a stereotactic
surgery program in West Africa can be expanded to include stereotactic endoscopy,
stereotactic craniotomy, functional neurosurgical procedures and radiosurgery.
The benefits from such a program will include, the acquisition of an accurate
histologic database for intracranial lesions, capability for neurophysiologic
research, enhanced medical education for medical students and neurosurgical
residents, clinical improvements in patient care and reduction of health care
costs.
ACKNOWLEDGEMENT
This work was presented in part at the 5th International Congress
on Minimally Invasive Neurosurgery, 2001. I gratefully acknowledge the invaluable
aid provided by A.A. Kelly, J. Asamoah, D. Moot, J. Arthur, D.Ampofo and E.
Narh, M.D.
REFERENCES
- Apuzzo MLJ, Chandrasoma PT, Cohen D, Zee CS, Zelman V: Computed imaging
stereotaxy: Experience and perspective related to 500 procedures applied to
brain masses. Neurosurgery, 1987;20:930-937
- Apuzzo MLJ, Sabshin JK: Computed tomographic guidance stereotaxis in the
management of intracranial mass lesions. Neurosurgery , 1983.12:277-285
- Bernstein M, Parrent AG: Complications of CT-guided stereotactic biopsy
of intra-axial brain lesions. J Neurosurgery 1994;81:165-168,
- Bosch DA: Indications for sterotactic biopsy in brain tumors. Acta Neurochir
1980.54:167-179,
- Bosch DA: Stereotactic Techniques in Clinical Neurosurgery: Berlin, Springer,
1986, pp145-156.
- Clarke RH, Horsley RV: On a method of investigating the deep ganglia and
tracts of the central nervous system (cerebellum). Br. Med J , 1906;2:1799-1800
- Coffey RJ, Lunsford LD: Stereotactic surgery for mass lesions of the midbrain
and pons. Neurosurgery 1985;17:12-18,
- Coffey RJ, Lunsford LD: Localization and biopsy of intracranial lesions
with computed tomography and magnetic resonance imaging. In Operative Neurosurgical
Techniques; Indications, Methods and Results ed Schmidek HH, Sweet WH, WB
Saunders Company, 1988; pp 463-474.
- Chandrasoma PT, Smith MM, Apuzzo MLJ: Stereotactic biopsy in the diagnosis
of brain masses : Comparison of results of biopsy and resected surgical specimen.
Neurosurgery 1989;24:160-165,
- Davis DH, Kelly PJ, Marsh WR, Kall BA, Goerss SJ: Computer-assisted stereotactic
biopsy of intracranial lesions. Appl Neurophysiol 1987;50: 172-177,
- Galloway RL, Maciunas RJ: Stereotactic neurosurgery. CRC Crit Rev Biomed
Eng 1990;18:181-205,
- Hood TW, Gebraski SS, McKeever PE, Veres JL: Stereotaxic biopsy of intrinsic
lesions of the brain stem. J Neurosurg 1986;65:172-176,
- Kelly, PJ: Stereotactic surgery: What is past is prologue. Neurosurgery,
2000 46: 16-27
- Kleihues P, Volk B, Anagnostopoulos J, Kiesssling M: Morphologic evaluation
of stereotactic brain tumor biopsies. Acta Neurochir Suppl 1984;33:171-181,
- Lee T, Kenny BG, Hitchcock ER, Teddy PJ, Palividas H, Harkness W, Meyer
CHA: Supratentorial masses: Stereotactic or freehand biopsy? Br J Neurosurg
1991;5:331-338,
- Lobato RD, Rivas JJ: Applications of CT-adapted stereotaxis for the diagnosis
and treatment of intracranial lesions. Acta Neurochir1987. 87: 14-21,
- Lunsford DL, Coffey RJ, Cojocaru T, Leksell D: Image-guided stereotactic
surgery: A 10 year evolutionary experience. Stereotact Funct Neurosurg 1990;54+55:
375-387,
- Maciunas RJ, Galloway RL, Latimer JW: The application accuracy of stereotactic
frames. Neurosurgery 1994;35:682-695
- Mundinger F: CT stereotactic biopsy for optimizing the therapy of intracranial
processes. Acta Neurochir Suppl , 1985;35: 70-74
- Neal JH, Van Norman AS: Transcerebellar biopsy of posterior fossa lesions
using the Leksell Gamma model stereotactic frame. Neurosurgery 1993;32:473-475,
- O'Neill KS, Dyer PV, Bell BA, Wilkins PR, Uttley D, Marsh HT: Is peroperative
smear cytology necessary for CT-guided stereotaxic biopsy? Br. J Neurosurg
1992.6:421-427,
- Revesz T, Scaravilli F, Coutinho L, Cockburn H, Sacares P, Thomas DGT: Reliability
of histological diagnosis including grading in gliomas biopsied by image-guided
stereotactic technique. Brain 1993; 116: 781-793,
- Ranjan A, Rajshekhar V, Joseph T, Chandy MJ, Chandi SM: Nondiagnostic CT-guided
stereotactic biopsies in a series of 407 cases: Influence of CT morphology
and operator experience. J Neurosurg 1993;79:839-844,
- Soo TM, Bernstein M, Provias J, Tasker R, Lozano A, Guha A: Failed stereotactic
biopsy in a series of 518 cases. Stereotact Funct Neurosurg 1996;64:183-196,
- Taratuto AL, Sevlever G, Picardo P: Clues and pitfalls in stereotactic biopsy
of the central nervous system. Arch Pathol Lab Med 1991;115:596-602,
- Thomas DGT, Nouby RM: Experience in 300 cases of CT directed stereotactic
surgery for lesion biopsy and aspiration of hematoma. Br J Neurosurg 1989;3:321-326,
Copyright 2002 - African Journal of Neurological Sciences
The following images related to this document are available:
Photo images
[ns02005t1-2.jpg]
| 
{kind=link}