 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 96(4) Mar. 2001, pp. 503-505 SHORT COMMUNICATION Comparison of Polymerase Chain Reaction on Fresh Tissue Samples and Fecal Drops on Filter Paper for Detection of Trypanosoma cruzi in Rhodnius prolixus PL Dorn/+, J Flores, B Brahney, A Gutierrez, R Rosales*, A Rodas*, C Monroy* Department of Biological
Sciences, Loyola University, 6363 St. Charles Ave., New Orleans, LA 70118, USA
*Escuela de Biología, Universidad de San Carlos, Guatemala, Central America
Received 3 July 2000
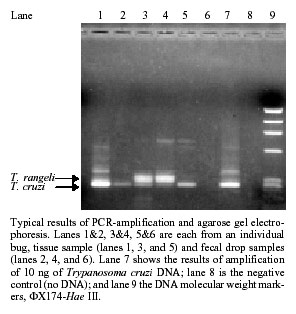
Code Number: oc01076 PCR detection of Trypanosoma cruzi in Rhodnius prolixus using fresh tissue or fecal drops on filter paper showed comparable results: 38.7% infection rate using the fresh tissue sample and 37.9% by dried fecal drop. Key words: Trypanosoma cruzi - Rhodnius prolixus - PCR PCR has shown to be more sensitive than microscopy in detecting Trypanosoma cruzi infection only in certain vectors (Brenière et al. 1995). In Guatemalan vectors, PCR is significantly more sensitive only for Rhodnius prolixus (Dorn et al. 1999) using primers (TC1 and TC2) complementary to the abundant kinetoplast DNA (kDNA). Detection of T. cruzi in Central America is complicated by the presence of the morphologically similar, but non-pathogenic, T. rangeli, which is also amplified by these primers; however, the size of the amplicons is sufficiently different to distinguish the parasites (Dorn et al. 1999). It should be noted that the PCR assay is heavily biased for the detection of T. cruzi over T. rangeli (Dorn et al. 1999). For the PCR, many investigators use the vector fecal drop as the template although some suggest that fresh tissue obtained by dissection of the bug is preferable (D'Alessandro-Bacigalupo & Saravia 1992). Results of PCR using these two types of samples have not been directly compared. In addition, for the fresh tissue sample, results of previous work suggested that a combination of rectum plus intestine would be the most useful anatomical site for detecting T. cruzi infection by PCR (Dorn et al. 1999), but this combination has not yet been tested. We report here results of a comparison of PCR detection of T. cruzi using either a fresh tissue sample (combined rectum plus intestine) or a dried fecal drop on filter paper. One hundred six R. prolixus vectors were collected from two villages in the southeastern region of Guatemala during the summer of 1997. Bugs were placed in individual plastic vials containing folded filter paper and left until they had deposited a fecal drop and then dissected. Bugs that died before depositing feces were discarded. The fecal drops were cutoff the filter paper and placed in individual microfuge tubes using scissors that were bleached between samples. Following collection of the fecal drop, a portion of the rectum and intestines was removed and placed in a microfuge tube for PCR analysis using bleached dissecting tools. The remainder of the rectum and intestines was dispersed in a drop of phosphate-buffered saline and examined under 400X magnification for approximately 2 min to search for hemoflagellates. For microscopy, the appearance of any hemoflagellate (T. cruzi or T. rangeli) was recorded as a positive result. Processing of the samples and the PCR was exactly as described (Dorn et al. 1999) and was identical for the fresh tissue and the fecal drop samples. Figure shows the results of a typical PCR comparing amplification of fresh tissue to dried fecal drop samples in three different bugs. The characteristic 280-bp T. cruzi band can be seen in lanes, 1, 2, 5, and 7, and the characteristic 320-bp T. rangeli band in lanes 3 and 4. By PCR using fresh tissue, 71/106 (67%) showed infection with either parasite, T. cruzi or T. rangeli and by PCR using the fecal drops, 81/103 (78.6%) showed infection with either or both parasites. By microscopy of these same insects, 45/106, (42.5%) of R. prolixus samples were infected with a hemoflagellate, either T. cruzi or T. rangeli or both. Therefore, PCR was significantly more sensitive than microscopy for detection of these parasites in R. prolixus using either the fresh tissue sample (c2=6.43, p<0.05) or the dried fecal drop on filter paper (c2=9.42, p<0.01). An additional advantage of PCR over microscopy is the ability to unambiguously identify T. cruzi, even in the presence of large amounts of T. rangeli. PCR using either vector sample, fresh tissue or fecal drops, identified approximately the same percentage of T. cruzi infections: fresh tissue (41/106, 38.7%) or the fecal drop on filter paper (39/103, 37.9%). Rates of T. rangeli infection are likely an underestimate since the assay fails to detect T. rangeli in the presence of >25% T. cruzi (Dorn et al. 1999). T. rangeli was detected slightly more using the filter paper samples (33/103, 32%) than the rectal tissue samples (29/103, 28.2%), which was not a significant difference (p>0.5). Very few mixed infections were observed (3/103, 2.9%, and only in the filter paper samples) which is likely an underestimation due to the bias of the assay for the detection of T. cruzi over T. rangeli (Dorn et al. 1999). For the majority of the bugs (59.2%), the tissue sample and the fecal drop sample showed identical results. For the case of a positive and a negative sample from the same bug, amplification of just one sample may signify inhibition of the PCR in the other. This was tested by "spiking", i.e., adding 1 ng purified T. cruzi DNA to the negative sample and re-amplifying by the PCR. Three of eight tissue samples that were negative for parasite infection (positive in the filter samples) showed an amplified product on PCR following spiking. Three out of three negative filter paper samples were amplified by the PCR when spiked. Thus, inhibition of the PCR reaction by something present in the tissue sample can explain why some of those samples did not show evidence of a parasite when the filter paper sample did. Inhibition does not appear to be an explanation for why the filter paper sample was negative when the tissue showed parasites. It may be that a parasite was just not present in that fecal sample because the drop was too small and lacked parasites (sometimes there was only one, very small drop) or the bug may not have been shedding that particular parasite at that time. This latter explanation was further tested by analyzing three or four sequential fecal samples from the same bug. Occasionally (2/16 of the bugs analyzed), intermittent shedding of parasites was observed. Rarely samples from one bug would show different parasites in the tissue and the filter paper samples, which may be explained by the colonization of the rectal wall by T. cruzi and not T. rangeli or an altered ratio of the two parasites which would permit detection of T. rangeli, even in the presence of T. cruzi. T. cruzi or T. rangeli was more prevalent in some regions than others. For example, in Las Palmas, a small percentage (4.2% of 48 tissue samples or 12.8% of 47 filter samples) of the bugs showed infection with T. rangeli and approximately half (56.3% tissue or 55.3% filter samples) of the bugs carried T. cruzi. La Prensa had a much lower level of T. cruzi infection (24.3% of 37 tissue or 22.9% of 35 filter samples) with higher rates of T. rangeli infection (54.1% tissue or 60% of filter samples). The T. rangeli infection rates may only appear higher in La Prensa when compared to Las Palmas because T. rangeli infection in Las Palmas may be masked by the higher rates of T. cruzi infection. The other villages had less than nine bugs per village, so vector infection rates were not analyzed. Thus, it appears that for the detection of T. cruzi in R. prolixus a fresh tissue sample or a dried fecal drop give comparable results by PCR. In addition, the results here confirm that PCR is significantly more sensitive than microscopy for the detection of T. cruzi in R. prolixus. ACKNOWLEDGEMENT To Robin DeVille for technical assistance. REFERENCES
[ Medline ] [ SciELO ] Copyright 2001 Fundacao Oswaldo Cruz Fiocruz The following images related to this document are available:Photo images[oc01076f1.jpg] |
| |||||||||

{kind=link}