 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 96(5) July 2001, pp. 635-640 Hepatitis B Infection among Patients Attending a Sexually Transmitted Diseases Clinic in Rio de Janeiro, Brazil Ledy HS Oliveira+, Isabel R Silva, Brunno LS Xavier, Silvia MB Cavalcanti Departamento de Microbiologia e Parasitologia,
Instituto Biomédico, Universidade Federal Fluminense, Rua Prof. Ernani
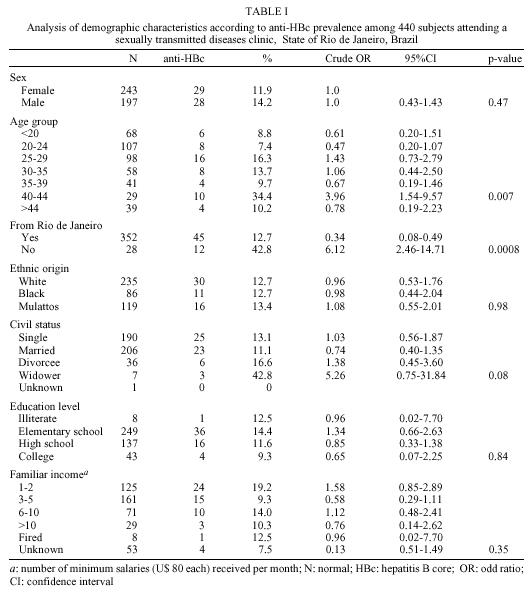
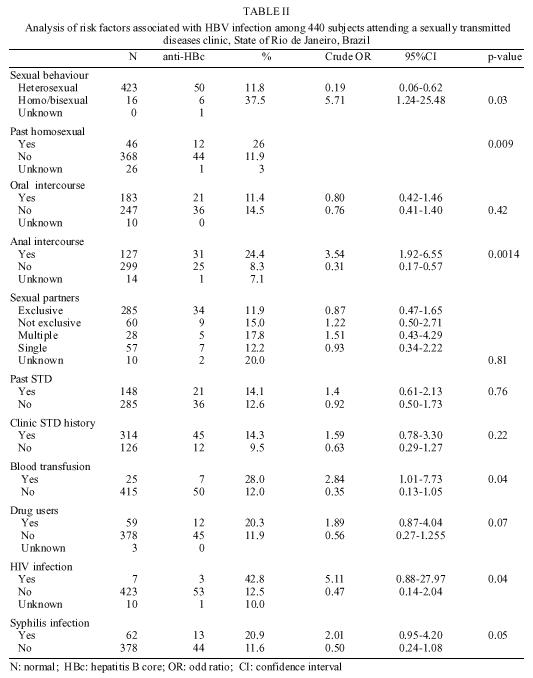
Melo 101, 24210 Niterói, RJ, Brasil Received 22 August 2000 Code Number: oc01096 Hepatitis B virus (HBV) has a low endemicity in Rio de Janeiro, Brazil. Sexual transmission must play an important role in this virus, but the prevalence and risk factors have never been properly investigated. The aim of this paper is to determine the prevalence and risk factors for HBV infection in patients attending a Sexually Transmitted Diseases Clinic of the Universidade Federal Fluminense, from the State of Rio de Janeiro, Brazil. In a retrospective study, HBV seroprevalence was investigated in 440 patients. Serum of each patient was assayed for antibodies against hepatitis B core antigen (anti-HBc), hepatitis B surface antigen (HBsAg) and antibodies against hepatitis B surface antigen (anti-HBs). Demographic and risk factor data were extracted from clinic notes. The overall seroprevalence of exposure markers for HBV (anti-HBc, HBsAg and anti-HBs) were 13%, 3.4% and 8.5% respectively. Homo/bisexual behaviour, anal intercourse, HIV infection, positive serology for syphilis and blood transfusion were predictors of the HBV exposure. Among demographic data, age and place of birth were associated with the anti-HBc seropositivity. Key words: hepatitis B - seroprevalence - sexual transmission Hepatitis B virus (HBV) is a common world-wide infection, committing over 2 billion of the individuals alive today at some stage of their lives (Davey 1996). The virus is found in high concentrations in blood, serum, and wound exudate; in moderate concentrations in semen, vaginal secretions, and saliva; and in low concentrations in urine, sweat, tears, and breast milk. The predominant routes of transmission vary according to the endemicity of HBV infection. In areas of low endemicity the sexual contact is the major route of transmission. Extensive studies regarding HBV sexual transmission have been conducted in low HBV endemic countries (Struve et al. 1993, Gilson et al. 1998). Heterosexuals who have unsafe sex with multiple partners and homo/bisexual men are the high-risk groups for sexual transmission (Margolis et al. 1991). Brazilian Southeast has been recently categorized as low HBV endemic area (Martelli et al. 1999). Rio de Janeiro, a state within Southeast region, has an overall hepatitis B surface antigen (HBsAg) prevalence about 2% in general population (Nogueira et al. 1990, Vanderborght et al. 1993). Most of adult infected may have acquired the virus by sexual route but risk factors for this way has not been properly evaluated. Screening for hepatitis B in sexual transmission diseases (STD) clinics is not considered as routine procedure. Reports with adolescents (Raffaelli et al. 1993, Porto et al. 1994), pregnant women (Duarte et al. 1997) and women attending a STD clinic (Miranda et al. 1999) have provided information about sexual transmission of hepatitis B in Brazil, but extensive studies with patients attending STD clinics are still incomplete. The aim of this study is to provide epidemiological data regarding association of sexual transmission of HBV and risk factors among patients attending a STD clinic from the State of Rio de Janeiro, Brazil. MATERIALS AND METHODS Participants - A retrospective study was developed with 440 patients attending the STD Clinic at Universidade Federal Fluminense, State of Rio de Janeiro, Brazil, over April to December in 1997. Demographic data (sex, age, place of birth, ethnic origin, civil status, education, and socio-economic conditions) and risk factors for HBV infection (sexual behaviour, oral or anal intercourse, sexual partners, drug abuse (intravenous or not), current and past STD history, syphilis seropositivity, HIV infection and past history of blood transfusion) were extracted from the clinical notes. Blood sample was taken of each patient at the time of the attending STD clinic. Test methods - Sera samples were tested for total antibodies to hepatitis B core antigen (anti-HBc), hepatitis B surface antigen (HBsAg) and antibodies to HBsAg (anti-HBs) by enzyme immunoassay (Organon Tecnika) according manufacture's instructions. Samples were considered positive if the test was repeatable reactive. Statistical analysis - Data were analysed using EPINFO 6.04 (Center for Disease Control and Prevention, Atlanta, GA, EUA, 1997) statistical software package. Odds ratio were presented with 95% confidence intervals (CI). The Chi-squared test assessed the significance between variables and serological status. Probability values less than 0,05 were considered significant. RESULTS Demographic finds - The sample comprised 243 females and 197 males with age range 14-72 years, average: 29 years (SD=9.1). Most of the patients (80%) were from the State of Rio de Janeiro (352/440). Among them, 53.4% (235/440) were white, 19.5% (86/440) had black, origin and 27% (119/440) were mulattos. The analysis of the relationships status revealed that 43.2% (190/440) were single, 46.8% (206/440) were married or had stable partner, 8.2% (36/440) were divorce and 1.6% (7/440) were widower. Considering the education level, 1.8% (8/440) were illiterates; 56.5% (249/440) had elementary school (completed or not); 31.1% (137/440) had high school (completed or not); and 9.7% (43/440) had college (completed or not). At the time of the survey, 28.2% (125/440) earned up till one or two living wages, 36.5% (161/440) earned from 3 to 5 living wages, 16.1% (71/440), earned from 6 to 10 living wages and 6.5% (29/440) earned up 10 living wages. One living wage is about 80 dollars. Eight (1.8%) of the patients were fired. Specific data - Among the patients, 95.4% related to have heterosexual life stile (177 males and 246 females) and 3.6% (15 males and one female) were homo/bisexual. However, 10.5% of the patients (39 males and 7 females) reported past homosexual relation. Oral and anal sex was a common practice in 41.6% (183/440) and 28.8% (127/440) of the patients, respectively. In relation to partnerships, 64.8% (285/440) had exclusive partner, 13.6% (60/440) had stable but not exclusive partner, 6.4% (28/440) had multiple partners, and 13% (57/440) were single. Past STD partners were related by 33.3% (85/440) of the people. Of the patients attending, 71.3% (314/440) had clinic symptoms of STD (syphilis, gonorrhoea, chlamydia, HPV infection, herpes, trichomonas, candidiasis). The attending motives of the remaining people were climaterium, STD partner's, rape, HIV serology, gynaecologic, colposcopic and peniscopic exam. Seven patients (1.6%) reported hepatitis episode and 5.7% (25/440) were submitted to blood transfusion in the past. Drugs were used by 13.5% (59/440) of the patients. After routine blood test, 1.6% (7/440) of the patients were found HIV seropositive and 14.1% (62/440) were syphilis seropositive. Serologic results - Anti-HBc marker was found in 13% (57/440), HBsAg in 3.4% (15/440) and anti-HBs in 8.5% (37/440) of the subjects. The HBsAg prevalence was 2.4% (6/243) in women, 3.9% (7/176) in heterosexual men and 6.6% (1/15) in homo/bisexual men. Among anti-HBc seropositive individuals, 8.3% acquired immunity to HBV. The overall prevalence of the exposure to HBV infection can be estimated from the prevalence of anti-HBc in serum. HBV infection and demographic variables are given in the Table I. The anti-HBc prevalence was associated with age and place of birth. The highest anti-HBc seropositivity was found in the 40-44 years old age group (OR 3.96 CI 1.54-9.57, p<0.05). The anti-HBc prevalence showed to be lower in the patients born in the State of Rio de Janeiro than in the group born outside. Positive anti-HBc status and specific data are showed in the Table II. The HBV prevalence was significantly higher in homo/bisexual men than in heterosexual men (OR=5.71, CI 1.24-25.48, p<0.05) or in women (OR=4.17 CI 1.20-14.5, p<0.05). A similar trend was observed in patients with past homosexual behaviour. Among the sexual practices, anti-HBc positivity was affected by anal intercourse (OR=3.54, CI 1.92-6.55, p<0.05). Although clinic symptoms of STD were not significant for anti-HBc positivity, this marker was associated with HIV infection (OR=5.11, CI 0.88-27.97, p<0.05) and syphilis seropositivity (OR=2.01, CI 0.95-4.20, p=0.05). Drug users (injecting or not) had higher anti-HBc positivity than non drug users (OR=1.89, CI 0.87-4.04), but this finding was not significant We have also found a significant association between anti-HBc positivity and blood transfusion (OR=2.84, CI 1.01-7.73, p<0.05). This association was independent of the sex related risk factors. DISCUSSION This study discloses information about demographic characteristics and sexual behaviour of individuals attending at a public STD clinic from the State of Rio de Janeiro. In our study we have detected a highly increase in hepatitis B seroprevalence among patients older than 20 years old. This finding is compatible with the fact that sexual activity is a major route of HBV transmission. Place of birth was also strongly associated to HBV infection. People who had born outside the State of Rio de Janeiro presented a significative rate of HBV prevalence. Most of these patients were from rural cities of the northeastern and probably had migrated under economic deprivation. Infectious diseases are a major concern to this condition. Although Silveira et al. (1999) has showed an association of higher seroprevalence with lower socio-economic status in Brazil, we did not find statistical significance between anti-HBc seropositivity and familiar income. It is well established that the epidemiology of HBV infection varies greatly according to geographic, demographic and risks factors. In areas of low and intermediate endemicity the sexual transmission plays an important role on the spray of the infection (Struve et al. 1993, Heng et al. 1995). Multiple sexual partners, sexual behaviour, anal intercourse, syphilis and other sexual diseases are consistent data to attribute the sexual hepatitis B acquisition (Schereeder et al. 1982, Rosemblum et al. 1990). The HBV positive patients attended in the STD clinic were constituted as an heterogeneous group having significative frequency of these indicators. The findings suggest sexual route of HBV in these patients based on association between hepatitis B, HIV and syphilis. There was no further association between HBV markers and multiple sexual partners or others STD diseases. Although the heterosexual transmission of HBV is related as more frequently than homosexual transmission (Alter 1990, Duarte 1992), recent studies in STD clinics (Stroffolini et al. 1997, Gilson et al. 1998) showed the opposite. In answering about homosexual behaviour, 3.6% of the sample related to be homo/bisexual. In a recent survey, 2.5% of the Brazilian people have homosexual practices (Ministério da Saúde 2000). However, 10.5% of the our sample related homosexual habits in the past. The degree of uncertainty in answering questions about sexual preferences may affect the assess of the investigation. Our dates are according to the last papers. HBV prevalence was at least three times more frequently in homo/bisexuals than in heterosexuals. Among the recorded markers, HBsAg positivity is considered as current HBV infection. The STD patients had a higher proportion HBsAg marker when compared to the local estimates. According to Martelli et al. (1999), the Southeast region present a 0.9% rate for HBsAg. The rate of HBsAg positivity remained high in subset of women (2.4%), heterosexual men (3.9%) and homo/bisexual men (6.6%). According Blumberg (1990), males exposed to HBV becomes HBsAg carries easier than females. Although not significative, among STD patients the HBsAg frequency was two times higher for male carriers. We also found a significant dependency between HBsAg status and HIV seropositivity (p<0.05). Patients blood transfused had significative association with anti-HBc marker. These patients have not reported other risk factors. Although blood control in the State of Rio de Janeiro is considered efficient, Martelli et al (1999) have already pointed out that a residual risk of transfusion hepatitis B is still present in Brazil and other South American countries. Six out of seven patients anti-HBc positive became immune to virus and one, HBsAg carrier. Most of information of HBV prevalence in Brazil is available from blood donors and interviews does not included questions about sexual behaviour. The results of this investigation contribute to trace the sexual route of HBV in our state. Therefore, HBV infection could be prevented through the STD control activities. Besides, the HBsAg prevalence detected in this population is up to above the recommended for vaccination by WHO (1988). Hence, patients attending STD clinics should be routinely screened in order to identify HBV exposure and those found seronegative should be advised to be vaccinated. ACKNOWLEDGMENTS To the Laboratório de Hepatites Virais, Instituto Oswaldo Cruz, for the kits to detect the HBV serological markers and to Dr Nubia K Almeida, Statistical Department, UFF, for statistical treatment assistance. REFERENCES
Copyright 2001 Fundacao Oswaldo Cruz The following images related to this document are available:Photo images[oc01096t2.jpg] [oc01096t1.jpg] |
| |||||||||

{kind=link}
{kind=link}