 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 96(7) 2001, pp. 987-996 Leishmanial Antigens in the Diagnosis of Active Lesions and Ancient Scars of American Tegumentary Leishmaniasis Patients Armando Schubach/+ , Tullia Cuzzi-Maya, Albanita V Oliveira, Alexandrina Sartori*, Manoel P de Oliveira-Neto, Marise S Mattos, Marcelo Lodi Araújo*****, Wilson Jacinto S Souza***, Fátima Haddad****, Maurício de A Perez, Raquel S Pacheco**, Hooman Momen**, Sérgio G Coutinho***, Mauro Célio de Almeida Marzochi, Keyla Belizia Feldman Marzochi, Sylvio Celso Gonçalves da Costa*** Centro de Pesquisa Hospital Evandro Chagas-Fiocruz,
Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil *Departamento de Microbiologia
e Imunologia, Universidade Estadual de São Paulo, Botucatu, SP, Brasil
**Departamento de Bioquímica e Biologia Molecular ***Departamento de
Protozoologia, Instituto Oswaldo Cruz-Fiocruz, Rio de Janeiro, RJ, Brasil ****Departamento
de Patologia, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, RJ,
Brasil *****Serviço de Endoscopia Peroral, Hospital Geral de Bonsucesso,
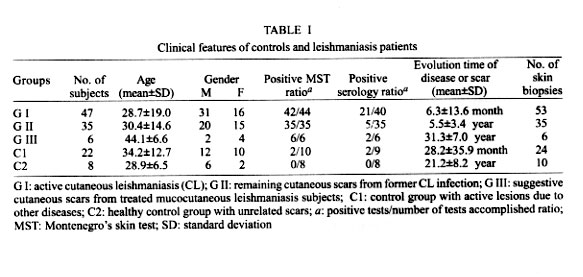
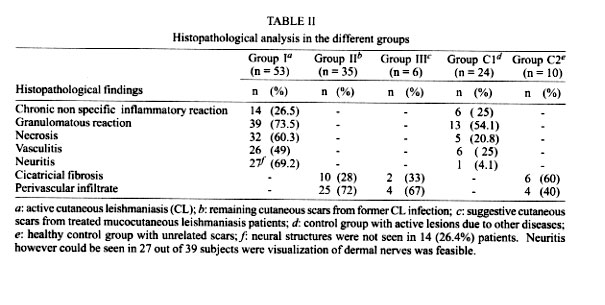
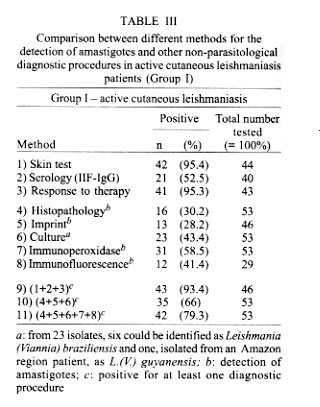
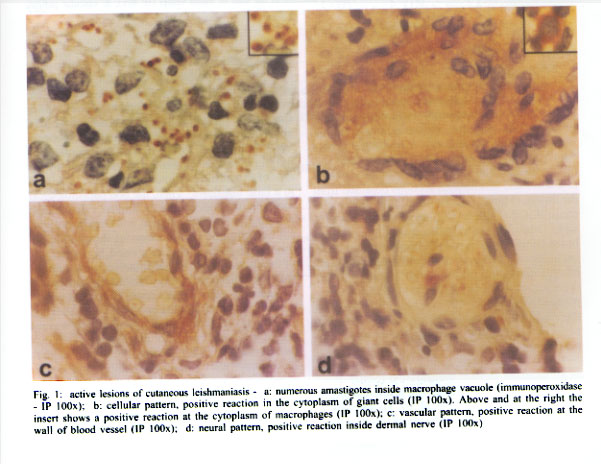
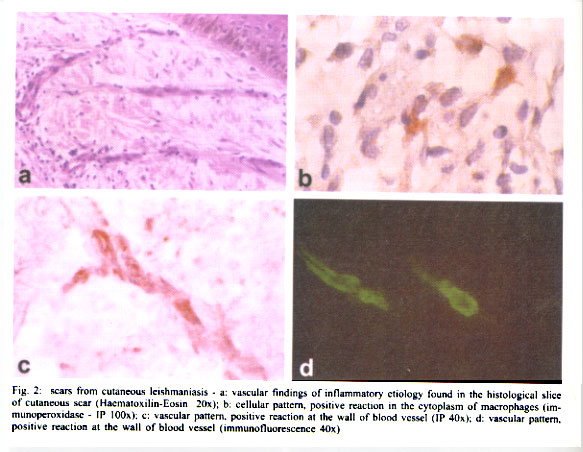
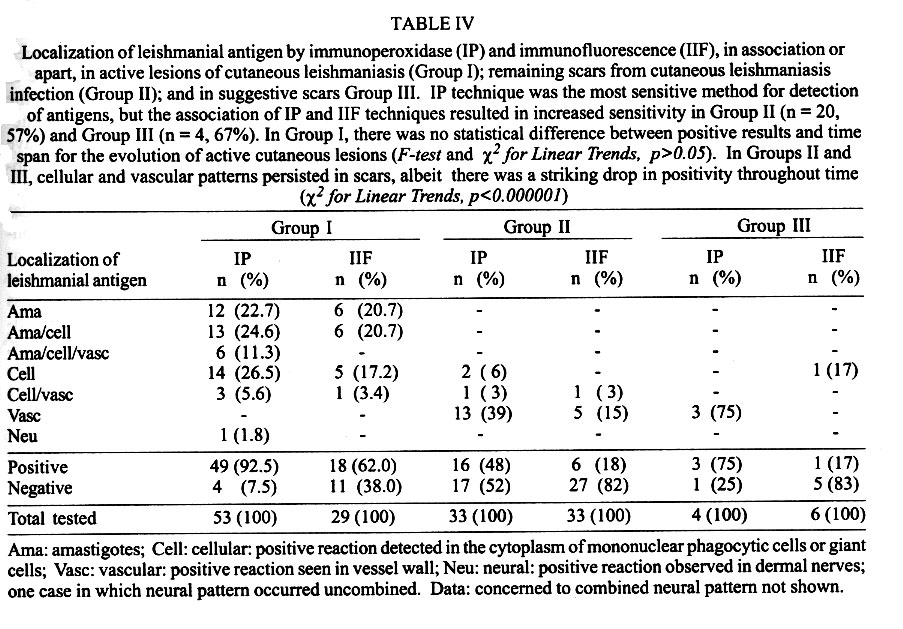
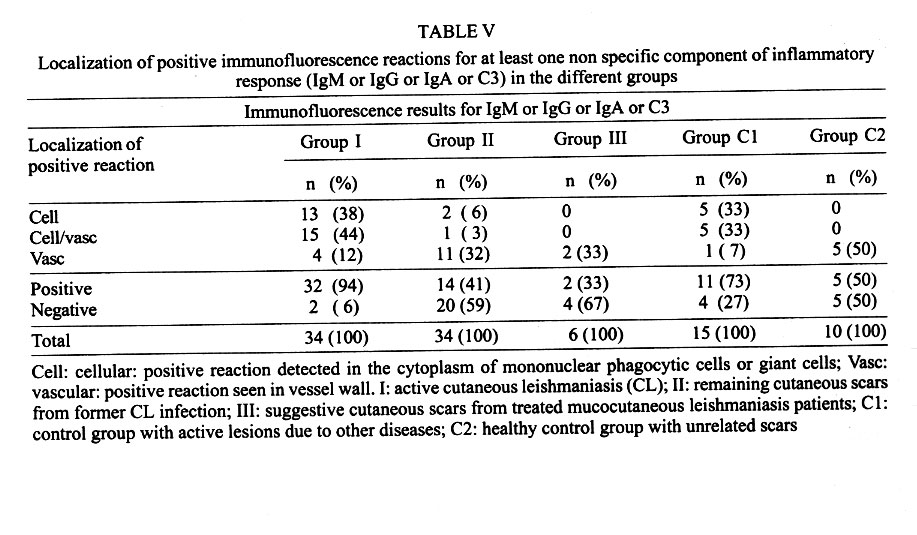
Rio de Janeiro, RJ, Brasil Received 12 September 2000 Code Number: oc01192 Cutaneous biopsies (n = 94) obtained from 88 patients with American tegumentary leishmaniasis were studied by conventional and immunohistochemical techniques. Specimens were distributed as active lesions of cutaneous leishmaniasis (n = 53) (Group I), cicatricial lesions of cutaneous leishmaniasis (n = 35) (Group II) and suggestive scars of healed mucosal leishmaniasis patients (n = 6) (Group III). In addition, active cutaneous lesions of other etiology (n = 24) (Group C1) and cutaneous scars not related to leishmaniasis (n = 10) (Group C2) were also included in the protocol. Amastigotes in Group I biopsies were detected by routine histopathological exam (30.2%), imprint (28.2%), culture (43.4%), immunofluorescence (41.4%) and immunoperoxidase (58.5%) techniques; and by the five methods together (79.3%). In Group II, 5.7% of cultures were positive. Leishmanial antigen was also seen in the cytoplasm of macrophages and giant cells (cellular pattern), vessel walls (vascular pattern) and dermal nerves (neural pattern). Positive reaction was detected in 49 (92.5%), 20 (57%) and 4 (67%) biopsies of Groups I, II and III, respectively. Antigen persistency in cicatricial tissue may be related to immunoprotection or, on the contrary, to the development of late lesions. We suggest that the cellular, vascular and neural patterns could be applied in the immunodiagnosis of active and cicatricial lesions in which leishmaniasis is suspected. Key words: American tegumentary leishmaniasis - Leishmania (Viannia) braziliensis - immunodiagnosis - scar - cured patients American tegumentary leishmaniasis (ATL) is endemic in Brazil. The most common species are Leishmania (Viannia) guyanensis, L. (Leishmania) amazonensis, and L. (V.) braziliensis, which has the widest geographical distribution and is the most prevalent, mainly outside the Amazon region in metropolitan areas, such as Rio de Janeiro (Marzochi & Marzochi 1994). Treated or not, after some months, cutaneous ulcers are prone to heal, leaving round, smooth, shiny scars, that are still described as atrophic, hairless and depressed with hypo or hyperpigmented areas (Marsden et al. 1984). It has been suggested that by an hematogenic parasite dissemination patients may develop the mucocutaneous form of leishmaniasis (MCL) (Martinez et al. 1992), at the same time as the cutaneous lesions, or from months to years after it has been healed (Walton et al. 1973). In these cases, besides the active mucous lesions, patients present one or more cutaneous scars, probably related to the primary infection. These concepts are so well established that patients with positive Montenegro's skin test (MST) and cutaneous scar are referred as "former cutaneous leishmaniasis" (CL) patients. Quite often, one can find references to the "scar of the primary cutaneous lesion" in patients with MCL (Jones et al. 1987, Aguilar et al. 1989). However, it would not be possible to make a secure diagnosis of old ATL cases by the conventional techniques. In the endemic areas of ATL other common diseases, such as bacterial infections, may also heal leaving a clinically indistinguishable scar and "typical scars" may be found both in MST positive and negative patients (Coimbra Jr. et al. 1996). The presence of spontaneous reactivation (Weigle et al. 1985), transmission by organ transplants (Golino et al. 1992) and cases in immunosuppressed patients (Coura et al. 1987) suggest the persistence of the parasites in humans (Rossell et al. 1992, Aebischer 1994). In these cases, diagnosis depends on the finding of parasites in the reactivated lesion, what is another evidence that scars may shelter amastigotes that could be responsible for active lesions, although the possibility of a new infection can not be excluded (Oliveira 1977, Saravia et al. 1990). Immunohistochemical techniques have proven successful in the diagnosis of ATL (Weigle et al. 1987). So we decided to verify the utility of these techniques for the identification of parasites in former CL scars and suggestive scars in previously healed MCL patients. In this paper we compared histopathological and immunohistochemical results found in active lesions from 47 CL patients with those from cutaneous scars in 41 previously healed ATL patients. MATERIALS AND METHODS Patients and controls - We studied 88 ATL Brazilian patients, distributed in three groups, according to the clinical form of the disease and presence or absence of active lesions. Group I: 47 patients with active CL; Group II: 35 patients previously treated for CL who presented scars; Group III: 6 patients treated for MCL and, at the time of their former disease, had presented suggestive cutaneous scars. Two control groups were included: Control group 1 (C1) – 22 patients with other cutaneous lesions in which a clinical and histopathological differential diagnosis with ATL could be established; and Control group 2 (C2) – Formed by 8 healthy volunteers who presented unrelated scars. After informed consent (to participate in the study) and submitting to a skin biopsy at the scar site, patients and controls underwent anamnesis, physical, dermatological and otorhinolaryngolo-gical examinations. The latter included anterior rhinoscopy by means of a nasal speculum, posterior rhinoscopy and laryngoscopy (Hopkins optics 0° e 90°). Other exams included MST, indirect immunofluorescence antibody test (IIF) and skin biopsy. Montenegro's skin test - Parasite antigens (leishmanin) containing 40 µg of proteic nitrogen/ml was obtained from the Instituto de Ciências Biológicas da Universidade Federal de Minas Gerais, Brazil (Melo et al. 1977). The magnitude of skin response was measured 48 h after intradermal injection of 0.1 ml of the antigen at the anterior face of forearm. The diameter of induration was measured in millimeters by outlining the indurated border with a ball-point pen and transferring to paper dampened with 70% ethanol for permanent record (Sokal 1975). Any induration of 5 mm or more was considered positive. All tests were performed and measured by a single observer. Serological reaction - An IIF was performed in order to detect anti-Leishmania antibodies. Goat IgG, conjugated with fluorescein isothiocyanate anti-human IgG was used (Sigma). The serial twofold dilution of the serum was done in phosphate-buffered saline (PBS). Antibody titers ³ 1:45 were considered positive. The fluorescence was evaluated with an epifluorescence microscope (Axiophot-Zeiss, Germany) (Souza et al. 1982). Biopsies - Incisional skin biopsy specimens from the borders of 128 active lesions or scars were performed throughout the previously defined groups (some patients were submitted to more than one biopsy). After careful sterilization of the biopsy site, local anesthesia with 2% lidocaine was carried out. The specimen was divided into three fragments: the first was fixed in 10% buffered formalin, embedded in paraffin and stained with Haematoxylin-Eosin, Grocott, Ziehl-Neelsen, and immunoperoxidase (Luna 1968). Before fixing in methanol, an imprint was performed and stained with Giemsa for microscopical examination (Luna 1968). The second was kept in sterile saline plus antibiotics (200 UI/ml penicillin and 200 µg/ml streptomycin) and kept at 4-8°C to the following day, when the specimen was triturated and then cultivated in enriched blood agar medium (NNN) in which LIT was added. Observation was carried out every 3-5 days, in order to detect the presence of Leishmania promastigotes for up to 30 days. The isolated parasites were characterized by isoenzyme electrophoresis (Momen et al. 1985) and restriction fingerprints of kDNA analysis (Pacheco et al. 1986). The third fragment was embedded on OCT medium (Ames Co. Elkhart, IN) and promptly frozen in liquid nitrogen. All specimens were kept at -70°C until immunofluorescence was performed. Anti-Leishmania serum - Anti-Leishmania serum was obtained in rabbits after two intramuscular inoculations (1 week interval) with 108 promastigotes emulsified in complete Freünd's adjuvant. We utilized a Leishmania isolated from a CL patient from the Southern region of Brazil and maintained in the laboratory. One week after the second injection the animals were inoculated three times intravenously on alternate days with 107 viable promastigotes. The rabbits were bled seven days after the last injection (Sartori et al. 1987). Antibody titres were tested by IIF (Shaw & Volles 1964). Anti-Leishmania serum was applied on histological sections at 1:160 dilution and reaction incubated overnight at 4-6°C. Anti-IgM, IgG, IgA and C3 antibodies - Lyophilized anti human IgM, IgG, IgA and C3 fluorescein conjugated antibodies (Behring Institute, France) were prepared according to manufacturer instructions and applied on histological sections at 1:20 dilution, for 20 min at room temperature. Immunoperoxidase technique - Histological sections were deparaffinized in xylene and rehydrated in alcohol and water. Inhibition of endogenous peroxidase was performed with a 30% hydrogen peroxide-methanol solution. Sections were incubated with goat normal serum (30 min at 37°C), and then with anti-L. (V.) braziliensis serum. Incubations with biotinylated goat anti-rabbit antibody and with avidin-biotin-peroxidase complex (ABC Vectastain Kit, Vector Laboratories, Inc., USA) were carried out for 30 min at 37°C. Positive reaction was detected with 3-amino-9-etil-carbazol solution. An histological sample with many Leishmania amastigotes was used as a positive control. Normal rabbit serum was applied instead of the anti-Leishmania serum in a negative control (Sartori et al. 1987). IIF technique - Frozen sections were fixed in acetone for 10 min, washed in PBS and incubated with rabbit anti-L. (V.) braziliensis serum , or with anti-IgG, IgM, IgA and C3 antibodies at 37°C for 30 min. Sections treated with anti-Leishmania serum were overlaid with goat anti-rabbit immunoglobulin fluorescein conjugated antibody (Vector Laboratories, Inc., USA) for 30 min at 37°C and mounted in glycerol. Positive and negative controls were similar to those performed in the immunoperoxidase protocol described above. Statistical methods - The F-test, Chi-square for linear trends and Chi-square paired test (Mc Nemar) were utilized in the statistical analysis. RESULTS Patients and controls - Data concerning the number of patients studied, their MST, IIF the disease or cutaneous scar evolution and number of biopsies performed, are presented in Table I. Most patients of Group I (39 out of 47) lived in Rio de Janeiro City. Lesions were present for less than 4 months in 37 cases (71.7%). Cutaneous ulcers were observed in 40 patients. Mucosal exam was normal in all patients. A good therapeutic response to different antimonial treatment protocols (Oliveira-Neto et al. 1997a, b, c) was observed in 41 patients; 4 of them abandoned treatment and 2 had no clinical improvement. Group II patients were from endemic areas of Rio de Janeiro City, where they still lived. The time elapsed after CL treatment varied between one and 14 years. A cutaneous atrophic scar was observed in all of them and no mucosal lesion was detected. The six members of Group III came from other Brazilian areas but were living in Rio de Janeiro. The time elapsed after MCL treatment varied between 5 and 12 years. All were asymptomatic, with no active mucosal lesions and presented cutaneous scars that could result from previous CL that spontaneously healed without any specific treatment, between 18 and 37 years ago. From the 22 patients of Group C1, 9 lived in areas of active ATL transmission, while 13 reported fortuitous visits to those areas. Active mucosal lesions together with cutaneous lesions were present in 5 patients. Twenty-four biopsies were performed and histopathological report was compatible with paracoccidiodomycosis (5 cases) , tuberculosis (4 cases), sporotrichosis (2 cases), granuloma annulare (2 cases), basal cell epithelioma (2 cases), hemangioma (2 cases), tuberculoid leprosy (2 cases), erythema induratum (1 case), cutaneous ulcer of sickle cell disease (1 case), eritema annulare centrifugum (1 case), lichen planus (1 case), and ulcerated histiocytoma (1 case). Of those, one patient in whom a diagnosis of paracoccidioidomycosis was made, presented IIF IgG = 1:45 and a MST = 30 mm. A second one, also with paracoccidioidomycosis, presented IIF IgG = 1:45; and a third patient , with tuberculosis, presented a MST = 6 mm. The eight healthy volunteers (Group C2) were health professionals living in non endemic areas of Rio de Janeiro. They had no clinical history of ATL and no mucosal lesions. Ten biopsies were performed, 8 of which in vaccinal (anti-smallpox ) scars and 2 in old traumatic scars. Histopathology and imprints - Histopathol-ogical exams were performed in all cases. Different patterns were identified. For the active lesions groups (Group I and C1), two different patterns were identified: (i) chronic non specific inflammatory reaction - diffuse infiltrate composed of lymphocytes, plasma cells, macrophages, granulocytes and cellular debris; (ii) granulomatous reaction - same pattern as mentioned above, associated with epithelioid cells and granuloma formation, frequently, with giant cells. Moreover, "vasculitis" (presence of inflammatory cells on the wall of blood vessels), "neuritis" (perineural inflammatory infiltrate, also observed in the vicinities of dermal nerves) and necrosis alterations were reported. For the cicatricial lesions (Group II, III and C2), observations indicated the presence of dermal fibrosis (dense connective tissue without others findings) and "perivascular infiltrates" (mononuclear cells around dermal vessels). Results are shown in Table II. Amastigotes were detected in tissue sections and in imprints in Group I (Table III), but not in the other groups. Leishmania culture - Results from Group I are shown in Table III. In two patients (5.7%) of Group II, treated 8 and 11 years before, respectively, cultures were positive and in one of them the isolated parasite was identified as L. (V.) braziliensis. Culture was negative in the other groups, for a 30 days period of observation. Anti-L. (V.) braziliensis serum immunoperoxi-dase staining - Four different patterns were identified: (i) amastigotes, seen only in Group I; (ii) cellular pattern: positive reaction detected in the cytoplasm of mononuclear phagocytic cells or giant cells; (iii) vascular pattern: positive reaction seen in vessel wall; and (iv) neural pattern: positive reaction observed in dermal nerves, seen only in Group I (Figs 1, 2). In Group I at least one of these patterns was detected in 49 out of 53 biopsies fragments (92.5%). Amastigotes, identified by visualization of their nucleus and kinetoplast or by their size and shape, were seen in 31 out 53 biopsies fragments (58.5%). The cellular and vascular pattern were present in 68% and 17% of the samples examined, respectively. The neural pattern was observed in 12 out of 47 (25.5%) tissue samples in which dermal nerves were present, and in 3 of them amastigotes were seen. Results of groups I, II and III are shown in Table IV. In the control groups immunoreaction was negative, except for 5 cases of paracoccidioidomycosis and one case of sporotrichosis in which yeast structures were positive. In all groups immunoreaction was negative when the primary antibody was replaced by normal rabbit serum. Anti-L. (V.) braziliensis serum immunofluorescence staining - The immunoreaction patterns described above were also seen in the immunofluorescence reaction, except for the neural pattern that could be obscured by the impossibility to actually perceive dermal nerves in the dark field (Fig. 2). In Group I, 18 out of 29 (62%) biopsies showed positive reaction. These results and those from Group II and III are listed in Table IV. Other 19 studied lesions of Group C1 and 10 scars samples of Group C2 were negative. Autofluorescence of fungal structures of Paracoccidioides brasiliensis was noted and not eliminated when normal rabbit serum was applied instead of the primary antibody. Anti-IgG, IgM, IgA and C3 antibodies immunofluorescence - Results are shown in Table V. Statistical analysis (Chi-square Paired Test - Mc Nemar) - In Group I, no correlation was found between: (i) inflammatory vascular alterations and the presence of Leishmania antigen (vascular pattern) (p < 0.003); (ii) the positive patterns found with the anti-Leishmania antibody and that found with anti-IgG, IgM, IgA and C3 antibodies (p < 0.008). However, when Group II and III were analyzed together we could not refuse those hypotheses (p > 0.05 and p < 0.03, respectively). DISCUSSION For the differential diagnosis in relation to other diseases such as leprosy, paracoccidioidomycosis, tuberculosis, sporotrichosis etc, parasitologic confirmation becomes necessary, including the identification of the parasite. However, this is not always possible, since L.(V.) braziliensis grows poorly in culture media, infects experimental animals with difficulty and appears in small numbers in smears and histological sections obtained from the lesions (Marsden 1986, Barral et al. 1987). Because it is difficult to find parasites in active lesions (Marsden 1986), indirect ATL diagnosis is based on epidemiological evidence as well as clinical aspects, MST, serology and histopathological examination. The magnitude of response to the specific treatment may also help to confirm the hypothesized diagnosis (Oliveira-Neto et al. 1988). In this study, indirect diagnosis was reached in 93.4% of the patients studied in Group I and that is a high percentage of positivity. The MST can be applied in ATL endemic areas as an index of disease transmission (Souza et al. 1992), while IgG IIF can show low levels of antibodies or be negative (Chiari et al. 1973), specially in one with a single cutaneous lesion of less than three months duration (Marzochi et al. 1980). On the other hand, as it was observed in Group C1, MST can be positive in persons with other diseases or that are even apparently healthy (Mendonça et al. 1986, Coimbra Jr. et al. 1996). In those conditions, blood antibodies can also be present (Camargo & Rebonato 1969, Walton et al. 1972). In addition, spontaneous healing of lesions that are not leishmaniasis, by the time of an equivocal antimonial treatment, could lead to a false diagnosis. Then, the non parasitological methods of diagnosis are of limited value. When parasites are not demonstrated, and there is an atypical evolution or an unsuccessful therapeutic response, diagnosis should be revised. Some patients of the current study, in that situation, were submitted to more than one biopsy. The biopsies performed in cutaneous scars did not result in reactivation in none of the cases studied up to 10 years after the study was concluded, in spite local trauma was reported to be responsible for reactivation of the disease (Netto et al. 1986). Because the clinical similarity between small CL scars and smallpox or its immunization injection scars (D'Utra e Silva 1915), we decided to include the last as control group (C2). In the lesions caused by L. (V.) braziliensis, the shortage of amastigotes, their partial degradation and presence of cellular dust often hamper demonstration of parasites in the tissue. Therefore other methods to reach the parasitological diagnosis are mandatory (Weigle et al. 1987, Brujin et al. 1993). In this study the immunoperoxidade technique was the most sensitive method for detection of amastigotes in active lesions and association of different methods resulted in increased sensitivity (Table III), as also demonstrated by others (Livni et al. 1983, Salinas et al. 1989). Even though, in 7 out of 47 patients of Group I, demonstration of parasites could not be done. In addition, amastigotes were found in dermal nerves in 3 out 12 active lesions in which the neural pattern was detected. These findings could be related to the fact that cutaneous ulcer is painless (Kubba et al. 1987, Satti et al. 1989). Neural structures were not found in the dense connective tissue of scar lesions. Although vascular and cellular pattern positivity have been previously described (Sells & Burton 1981, Ridley & Ridley 1986, Salinas et al. 1989, Sotto et al. 1989) their possible value in the diagnosis of the disease was not stressed. In our work the cellular, vascular and neural patterns permitted that immunoperoxidade technique positive results reached from 58.5% (amastigote) to 92.5% in Group I. However, three patients still would remain without demonstration of amastigotes or their antigens. PCR reaction was performed in two of these three negative cases. Positive PCR was obtained both in the active and in the 5 years old scar in one patient. In the second one all performed exams, including PCR, were negative, and there was no response to antimonial therapy. In spite of a strong epidemiological history (9 persons in the family group have had leishmaniasis in the past 2 years), diagnosis of ATL in that patient is not likely. The third patient, in whom PCR was not done, presented positive MST and a 8 years old cutaneous ulcer that healed after 30 days treatment with N-methyl-glucamine. The suggestion for cellular and vascular patterns application in the diagnosis of ATL is coherent with some physiopathologic events. Macrophages are host cells for Leishmania parasites but also participate in the defense against them (Mauel 1982, Ridley & Ridley 1986). The granular positive material found in their cytoplasm should correspond to Leishmania antigens, as that seen in areas of necrosis (Ridley & Ridley 1984, 1986). Although antigen, immunoglobulin and complement were detected in the current study, statistical correlation was not achieved between the presence of antigen and inflammatory cell infiltrate or immunoglobulin/complement in vessel wall. Inflammatory vascular alteration (Magalhães et al. 1982, Veress & El Hassan 1986) and presence of free leishmanial antigen, immunoglobulins and complement were previously described in skin biopsies of ATL (Ridley & Ridley 1984, 1986). The authors proposed that immune complexes would be formed in situ and that the soluble antigenic component would localize in the endothelium. In the present report it was found an anti-Leishmania IgG-IIF = 1:45 in 2 patients with paracoccid-ioidomycosis. In one of them, the MST was also positive and a co-infection Leishmania-Paracoccidioides could be suggested. However only fungal structures were positive in their biopsies and none of the other immunostaining patterns were detected. Others (Salinas et al. 1989) described cross reactivity with P. brasiliensis. The 41 former ATL patients from which scars were studied, had a long lasting positive MST response after the clinical cure. Beside the finding of 2 (5.7%) positive cultures in Group II (Schubach et al. 1998b), persistence of parasite antigen was demonstrated in 21 (60%) out of 35 CL scars (Group II) and in 4 (66.6%) out of 6 suspected scars of MCL (Group III). In another study (Schubach et al. 1998a) 10 patients of Group I were included. They were rebiopsed between 48 days and 5 years after antimonial therapy and healing of the lesions. Leishmania DNA was demonstrated in the 10 biopsies of active lesions and in 6 of the respective scars. Considering that all patients were clinically cured up to 14 years after treatment, it is attractive to hypothesize that persistence of parasite in the healed scar is related to a mechanism of maintenance of the immune response. This could have provided a sufficient protection avoiding the appearance of new clinically detected lesions. The presence of amastigote, cellular, vascular and neural patterns in the same active lesions contrasts with the predominance of isolated cellular, or more often, vascular patterns seen in scars. It is likely that there is a dynamic and intense process of amastigotes destruction and subsequent antigen processing in active lesions, while in scars, the antigen keep still linked to phagocitic mononuclear cells or endothelial cells for many years after healing. Alternatively, as suggested by the finding of positive cultures in CL scars, there could be a state of equilibrium between host and parasite in which a light inflammatory response would allow survival of amastigotes sufficient to sustain the process (Müller 1992, Schubach et al. 1998b). Others papers reinforce this view (Bogdan et al. 1996, Stenger et al. 1996, Bogdan & Röllinghoff 1998). Such mechanisms, possibly related to reinfection (Saravia et al. 1990) due to repeated phlebotomine bites in former patients that kept living in ATL endemic areas, could have contributed to the maintenance of the immune response. The observation that disease duration would be an important factor in the determination of magnitude of the cellular immune response (Carvalho et al. 1985) suggests that the hyperactivity observed in MCL patients would be related to the fact that, in this form of the disease, the immunological stimulus would persist for a longer time than in CL. Once mucosal lesions can appear many years after the healing of cutaneous lesions (Walton et al. 1973), CL patients apparently cured, even for many years, could be in an intermediary phase of the natural evolution process toward MCL, or , alternatively, could be in a balance point that determines protection most of the time, and that just some individuals would evolve to the MCL. The epidemiological importance of clinically cured patients that keep living in endemic ATL areas is a subject rarely studied and with a difficult approach. The finding of viable infective parasites (Schubach et al. 1998b), Leishmania DNA (Schubach et al. 1998a) and antigen in cicatricial lesions and Leishmania DNA in the blood (Guevara et al. 1993) of clinically cured ATL patients could be related to immunoprotection or, on the contrary, to the development of later lesions. This finding also raises the possibility that these patients could play a role as a source of infection in the transmission cycle of the disease (Marzochi & Marzochi 1994). Finally, these findings also point towards the perspective to perform a retrospective diagnosis of ATL, starting in a suspicious cutaneous scar. ACKNOWLEDGMENTS To Marco Antônio G Botelho and Alcina F Nicol for technical support; Dr Mauro Tendrich for advice; Genilton José Vieira and Rodrigo da Cunha Mexas for photographic support; and Heloisa Diniz for artistic support. REFERENCES
Copyright 2001 Instituto Oswaldo Cruz - Fiocruz. The following images related to this document are available:Photo images[oc01192t5.jpg] [oc01192t3.jpg] [oc01192t2.jpg] [oc01192f2.jpg] [oc01192t4.jpg] [oc01192t1.jpg] [oc01192f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}