 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 96(8) 2001, pp. 1033-1042 The Search for New Antimalarial Drugs from Plants Used to Treat Fever and Malaria or Plants Ramdomly Selected: a Review Antoniana U Krettli/+, Valter F Andrade-Neto/*, Maria das Graças L Brandão**, Wanêssa MS Ferrari Centro de Pesquisas René Rachou-Fiocruz,
Av. Augusto de Lima 1715, 30190-002 Belo Horizonte, MG, Brasil *Departamento
de Parasitologia, ICB **Laboratório de Farmacognosia, Faculdade de Farmácia,
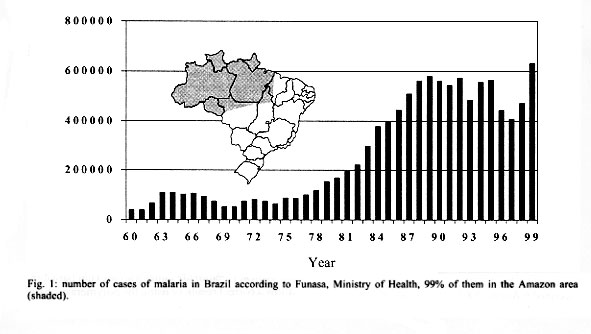
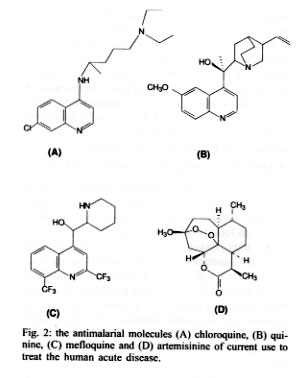
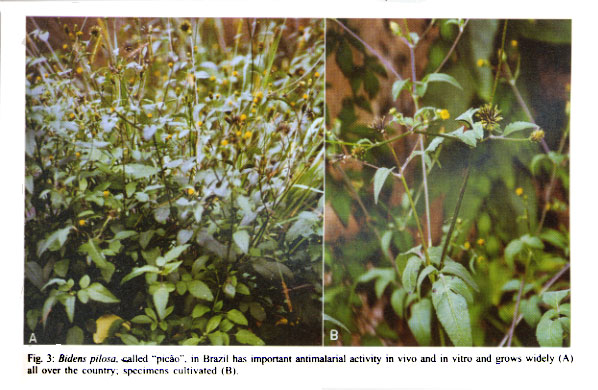
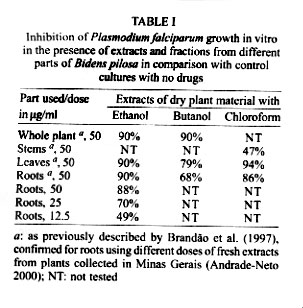
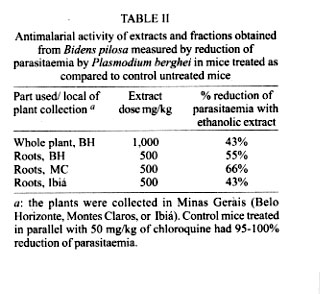
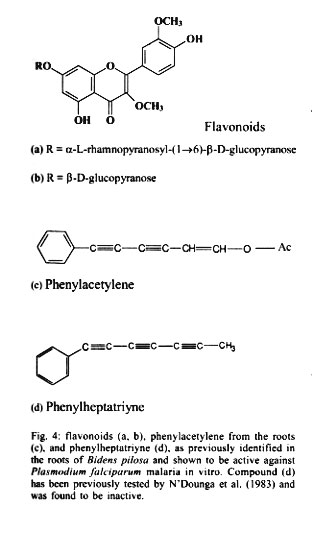
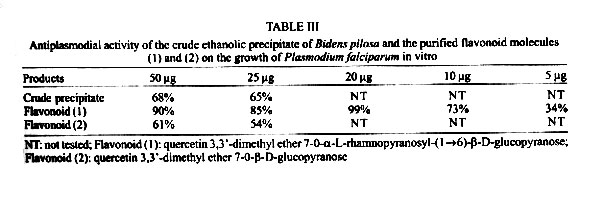
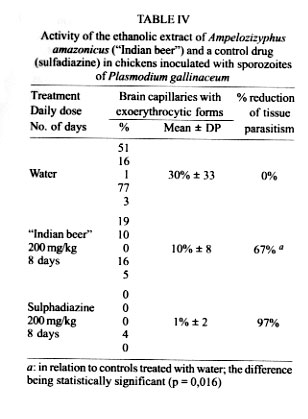
Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brasil Received 16 April 2001 Code Number: oc01201 In this review we discuss the ongoing situation of human malaria in the Brazilian Amazon, where it is endemic causing over 610,000 new acute cases yearly, a number which is on the increase. This is partly a result of drug resistant parasites and new antimalarial drugs are urgently needed. The approaches we have used in the search of new drugs during decades are now reviewed and include ethnopharmocology, plants randomly selected, extracts or isolated substances from plants shown to be active against the blood stage parasites in our previous studies. Emphasis is given on the medicinal plant Bidens pilosa, proven to be active against the parasite blood stages in tests using freshly prepared plant extracts. The anti-sporozoite activity of one plant used in the Brazilian endemic area to prevent malaria is also described, the so called "Indian beer" (Ampelozizyphus amazonicus, Rhamnaceae). Freshly prepared extracts from the roots of this plant were totally inactive against blood stage parasites, but active against sporozoites of Plasmodium gallinaceum or the primary exoerythrocytic stages reducing tissue parasitism in inoculated chickens. This result will be of practical importance if confirmed in mammalian malaria. Problems and perspectives in the search for antimalarial drugs are discussed as well as the toxicological and clinical trials to validate some of the active plants for public health use in Brazil. Key words: antimalarial drugs - plant extracts - human malaria - Plasmodium falciparum - ethnopharmacology MALARIA IN THE WORLD AND IN BRAZIL Malaria is a disease caused by Apicomplex protozoans, represented by 150 species of Plasmodium, transmitted by the bites of mosquito vectors to man, simians, rodents, birds, and reptiles. Malaria is present all over the tropics where four species infect humans, P. falciparum, P. vivax, P. malariae and P. ovale. Over 90% of cases occur in sub-Saharan Africa, causing over two million deaths each year with high mortality among children (WHO 1997). Malaria is also endemic in Southeast Asia, in Central and South America and Oceania. After the African countries, India and Brazil are presently the regions of highest endemicity in the World (WHO 1997). Three Plasmodium species occur in humans in Brazil: (i) P. falciparum, the most deadly if not treated; (ii) P. vivax, the most prevalent causing about 80% of the current cases, according to the Ministry of Health reports, and (iii) P. malariae, of lowest prevalence, presently under-diagnosed in Brazil due to the method used, the Giemsa stain thick blood smear. This method of blood concentration is ideal for malaria diagnosis being highly sensitive and specific, as reviewed by Ávila and Ferreira (2000). Misdiagnosis of P. malariae as P. vivax does occur unless the typical small mature P. malariae schizonts are found. Although treatment is successful with chloroquine for both species of parasite, P. vivax requires also a 14-day treatment with primaquine to prevent late relapses caused by liver hypnozoites. In addition, resistance of P. vivax to chloroquine and mefloquine has been demonstrated in Brazil (Alecrim et al. 1999). A more precise specific diagnosis requires the thin blood smear, and it should be ideal to implement it as a routine. Although adding a thin blood smear for malaria diagnosis will be more work, and more expensive, it seems regrettable missing most P. malariae cases in Brazil. In the thin blood smear the typical P. malariae equatorial asexual parasites allow a correct result, or using the polymerase chain reaction (PCR), non-practical in routine tests. A semi-nested PCR in blood of 96 malaria patients from Rondônia, Western Brazilian Amazon, showed 10% positive for P. malariae (Cavasini et al. 2000), none of which were identified by local microscopists, in spite of being highly trained in malaria diagnosis; therefore, there is a technical limitation of the thick blood smear test. The total number of acute malaria cases in Brazil is on the increase in endemic areas (Fig. 1), 99% being transmitted in the Amazon region. This reflects the social-economic decline of the rural south and east, with consequent waves of migration of workers to mining and agricultural projects in the north, where a larger population is exposed to endemic transmission. Transmission has never been interrupted in the Amazon where the waves of immigrants in the last decades, mostly non-immune individuals from areas where there is no malaria, have aggravated the situation. In addition, drug resistance of P. falciparum (reviewed in Zalis 2000) and P. vivax (Alecrim et al. 1999) has made control difficult. During the malaria eradication campaign, coordinated by the WHO and the Brazilian government, transmission of the disease was eliminated in most areas of the country outside the Amazon region. During the 70's about 70,000 cases of malaria occurred yearly a number risen gradually to 610,000, as shown in Fig. 1. As previously mentioned, although, the exposure of non-immune immigrants is responsible for the increase transmission, in one locality, Serra Pelada, where 20 thousand men used to dig for gold, malaria has never been a problem. This may be attributed to government control of gold mine and prompt treatment of those acutely ill which interrupted vector transmission. Migration from the Amazon region to other parts of Brazil has created new foci of transmission, which are likely to cause spread of the disease if not promptly controlled. For example, in the state of Minas Gerais, 14 new foci with autochthonous cases of malaria have been registered in the last decades. One of them occurred near Mantena, in the eastern part of the state never reported before as a malarial region. Over 100 individuals were detected in this locality, in 1989, as P. vivax positive by blood smear, originated apparently from a single imported case coming from southern of the state of Pará. Transmission was promptly eradicated by chloroquine and primaquine treatment of all positive cases in addition to prophylactic treatment of their families and neighbors, indoors inseticide spraying followed by a close surveillance throughout the succeeding months. This was one of the largest malaria foci detected outside the endemic area, and took about two months to be eradicated by the National Health Foundation - Funasa of the Ministry of Health. We had the opportunity to study the immune response to sporozoite, and to blood stage antigens in the area, after six months and again, up to seven years later, and no new cases were ever detected (Fontes et al. 1991, Braga et al. 1998). Part of these data have been published before (Krettli et al. 2001). THE MALARIAL CYCLE AND CHEMOTHERAPY The intrinsic characteristics of the disease, related to the conditions of transmission contribute to the difficulty in controlling malaria in Brazil. Primary factors are the complexity of the parasite life cycle, the absence of vaccines, drug resistance, and, the non-availability of prophylactic drugs. Secondly, the sporogonic cycle of the parasite in the Anopheles vector is rapid, completed in less than two weeks in the ideal conditions of temperature and humidity, like in the Amazon region, where the vectors abound in the extensive water collections. Thirdly, most houses have no screens and many are just open shelters, canopies covered with plastic or leaves and without walls, making it difficult to fight the mosquitoes with insecticides. In places where houses have walls, indoor spraying with insecticides helps transmission control. The use of insecticide impregnated bed nets, which decreased mortality rates in Africa, should help malaria control here, but they have not been tested in the Amazon. When the infected mosquito bites the vertebrate, the inoculated sporozoites migrate to the liver and invade the hepatocytes by mechanisms still not completely clear (Krettli & Miller 2001). A sporozoite generates about 30,000 new parasites in the case of P. falciparum or 10,000 in P. vivax. In the case of P. vivax, slow developing sporozoites, named hypnozoites, remain for months in the liver inducing new relapses of the disease with renewed patent parasitemia up to two years after initial infection. There is only one drug commercially available to destroy hypnozoites, primaquine, whose use prevents late relapses. Primaquine is also active against gametocytes and a single dose given to the host, from whom the blood meal is taken, totally inhibits the sporogonic malarial cycle in the vector (Gwadz et al. 1983). This model, useful for evaluating new anti-relapsing drugs to replace primaquine, was applied in our studies to test a popular prophylatic drug called "Indian beer", but it proved to be unable to inhibit sporogony (Carvalho et al. 1992, 1997), as discussed later. Fourteen consecutive daily doses of primaquine are required to prevent P. vivax relapses, which in the field is not practical, besides being toxic. Primaquine thus needs to be replaced by another drug not yet available, which represents one of our research goals in experimental chemotherapy with one Amazonian plant. In human malaria only the asexual blood stages (late trophozoites and schizonts) result in pathology causing the disease symptoms which appear about two weeks after the sporozoite inoculation. Symptoms are mainly headache, periodically recurrent high fever (every 48 to 72 h), myalgia , anemia, hepato- and splenomegaly. Neurological symptoms occur and may result in death in the case of severe P. falciparum infection, being caused by parasite sequestration and blockage of blood flow in small vessels of the brain. If treatment is not promptly performed, the disease caused by P. falciparum can lead to death, specially in acute primary infections. Treatment and control of the disease rely mainly on antimalarial schizonticidal drugs; new ones are urgently needed due to drug-resistance. PLANTS AS ANTIMALARIAL DRUGS - HYSTORY Most of the drugs currently available to treat malaria are quinoline derivatives modeled on the quinine molecule, found in the bark of Cinchona spp. trees found in high altitudes of South America. This genus is said to have been named after the Spanish Countess of Chinchón who was successfully treated with the powdered bark (Garnham 1966). In the XVI century, the plant bark and seeds were taken to Europe by the Jesuits and used for centuries to treat human malarial with efficacy. Cinchona plantations were established in Java and, until the Second World War, were the source of quinine. The quinine molecule inspired the synthesis of chloroquine and this drug became the chief replacement for quinine, during the Second World War. Chloroquine was close to the ideal antimalarial drugs and was used for decades due to its high efficacy against all species of malaria parasites, its low toxicity, low cost and high tolerance; it is still widely used to treat malaria in areas where notable drug resistance has not yet appeared. The structures of some currently used antimalarial drugs are shown in Fig. 2. Among the modern antimalarial compounds isolated from plants artemisinine is the most important one at present, being discovered and characterized by Chinese scientists. This substance (Fig. 2) comes from Artemisia annua L., a plant used for thousands years to treat malaria according to the Chinese Materia Medica. The isolation of artemisinine has inspired many research groups, including our own, since the early 80's, to look for new antimalarial drugs from plants. We then began our search based on popular knowledge or ethnopharmacology, rather than randomly, (Bote-lho et al. 1981/82, Brandão et al. 1985). MATERIALS AND METHODS Previously, we had tested synthetic antimalarial drug; hundreds from Hoffman la Roche, of which eight were active (Krettli & Brener 1968, Brossi et al. 1971, 1973); others were molecules modified from partly active compounds at the University of São Paulo (Korolkovas et al. 1978). Later, we tested extracts from over 300 plants randomly collected and three were found to be active, a rather low degree of success (Carvalho 1990, Carvalho et al. 1991). In a collaborative program with several groups of chemists in Brazil, we then focused tests of antimalarial drugs on medicinal plants used to treat fever, malaria and liver disorders believed to result from the disease, guided by previously published works on medicinal plants and in interviews on the malaria endemic areas in the Amazon region. The methods and approaches used to prepare and test these plants for antimalarial activity have been described previously (Brandão et al. 1985, 1992, Carvalho et al. 1991, 1997). The studies have aimed at the recovery of the extensive popular knowledge of the plants used to treat malaria in the Amazon region. In collaboration with a Social Sciences Research Group, (Cedeplar, UFMG ) over 8 thousand people were interviewed, most of whom had migrated recently to the Amazon region to work in mining or agricultural projects (Brandão et al. 1992). Ethanol, butanol, hexane and chloroform extracts were provided for the antimalarial assays, from the 70's onwards, first by the Natural Products Research Centre - NPPN of the Federal University of Rio de Janeiro (Benjamin Gilbert, now at Fiocruz), followed by the Pharmacy School, São Paulo University, in Ribeirão Preto (David dos Santos Filho and João Luis Callegari Lopes), from groups the Chemistry Department, Federal University of Minas Gerais-UFMG (Alaíde B Oliveira, Delio S Raslan and Tanus J Nagem). More recently the Institute of Chemistry, Federal University of Alagoas (A Euzébio and Marilia O Fonseca Goulart), the Department of Pharmacology, EPM, Federal University of São Paulo (Antonio J Lapa), and the local of Chemistry Laboratory, CPqRR-Fiocruz (Carlos Zani and co-workers) started to collaborate and continue as collaborators until now. The collected plant material was classified and used to prepare extracts which were tested in vitro against P. falciparum blood stage cultures. When sufficient amounts were provided, in vivo tests using P. berghei in mice were performed in parallel. In vivo tests are more practical, more rapid and less expensive then in vitro cultures, but not all antimalarial drugs are active in the P. berghei mouse model (Ferreira-da-Cruz et al. 2000). Also, the in vivo model requires significantly higher amounts of drugs, as compared to the in vitro assays, about 1g of extract per test. All extracts or molecules were tested in comparison with positive control drugs, represented by the standard antimalarials chloroquine, in parallel with untreated control cultures in medium only (control of parasite growth). For the in vivo tests, Swiss albino adult mice were infected with known numbers of blood parasites, randomly distributed in cages (3-4 mice per group), treated via oral during four consecutive days, starting one day after parasite inoculation. Blood smears were collected on days 5 and 7, fixed with methanol, stained in Giemsa and microscopically read under codes. Antimalarial activity was based on percentage of parasitaemia reduction caused by the test or the reference drugs, in relation to the average parasitemia observed in the non-treated mice. Mortality was monitored daily until the control mice died, another parameter of drug activity. RESULTS AND DISCUSSION In contrast with only 1% active plants among 300 randomly selected species which were tested, nearly 20% were found to be active among less than 50 plants based on traditional knowledge, identified up to the present. Antimalarial activities were observed initially with hexane and/or ethanolic extracts of Esenbeckia febrifuga ("três folhas"), Boerhavia hirsuta ("pega pinto"), Lisianthus sp., Acanthospermum sp., A. australe ("carrapicho"), Vernonia sp. and Tachia guianensis ("caferana") (Carvalho 1990, Carvalho et al. 1991). Tachia is used in the Amazon region as an antimalarial drug. Activities were promising but the plant extracts rarely reduced parasitaemia to a degree equivalent to chloroquine tested in paralel. Attempts to isolate and identify purified components from the active plants were disappointing. It could be related to difficulties in purifying glycosides (Lisianthus) or to non-retention of the initial activity (Vernonia sp. and other plants) in the purified fractions (Zani et al. 1997). The instability of purified substances was shown in the case of Bidens pilosa (Brandão et al. 1997) as discussed below. Stabilization of active components is being examined in some cases. Plants like Cecropia glaziouvii (colaboration AJ Lapa, Federal University of São Paulo), Bidens sp. and T. guianensis, in which significant antimalarial activity was found, are worthy further studies. Another group of plants, tested on the evidence of folkloric use, were the so called "false cinchonas" i.e. Deianira erubenscens, "fel-da-terra" (Gen-tianaceae), Strychnos pseudoquina, "quina-de-cerrado" or "quina-de periquito" (Loganiaceae) and Remijia ferruginea, "quina-da-serra" or "quina-do-Brasil" (Rubiaceae). They are popularly used to treat malaria in some areas but they were all found to be inactive and toxic in mice except for R. ferruginea, which had a borderline activity (Andrade-Neto 2000). New tests will be carried out with R. ferruginea before rejecting it. The bark of the true Cinchona species (C. calisaya and C. succirubra, Rubiaceae), not tested in our laboratory, cures malaria due to the presence of quinine (Fig. 2), a molecule characterized by Pelletier and Caventou in 1820. The inactive plants named "quinas" after the active cinchona, all have bitterness in common which probably led to their mistaken use. Bidens pilosa A POTENTIAL SOURCE OF NEW ANTIMALARIAL DRUG The most promising plant based on ethnoparmacology so far tested in our laboratory has been B. pilosa, called "picão", which widely grows in Brazil (Fig. 3). It is used all over the tropical and sub-tropical world where it is attributed anti-inflammatory, diuretic, antirheumatic and antibiotic activities being also used against diabetes and hepatitis (N'Dounga et al. 1983). In the Amazon region, the roots and aerial parts of Bidens sp. are used as an antimalarial drug and to treat liver complications believed to result from the disease. We first tested two species that are prevalent in Brazil, B. pilosa and B. bipinnatus and found both active. Later, we tested other species collected in Africa as well as in European countries (kindly supplied to MGL Brandão in Germany). The ethanolic and methanolic extracts of most Bidens species tested were very active (Brandão et al. 1997). The percentage of reduction of parasitaemia in P. falciparum cultures in vitro, caused by B. pilosa extracts, was mostly very high (Table I). The number and the aspect of the surviving parasites at day 4 of culturing with the drugs were observed in the blood smears. Lower parasitaemia occurred with most extracts of Bidens sp. as compared to that found in blood cultures in culture medium only. We consider a drug active when the percent reduction of parasitaemia is higher than 30% (Carvalho et. al 1991). Ethanol, butanol and chloroform extracts of B. pilosa are active at relatively low concentrations. Ethanolic extracts of B. pilosa prepared from leaves, roots and the whole plant were also tested in mice infected with P. berghei showing consistent activity. Regarding the root extracts, a more significant activity was confirmed in further studies (Andrade-Neto 2000) with plants collected in three different regions of the state of Minas Gerais (Table II). Antimalarial evaluation of nine species of Bidens, performed in parallel tests, showed intense activity in seven species, partial activity in one and no activity in one species (Brandão et. al 1997). The ranges of activities observed in vitro using 50 µg/ml varied from over 80% (B. frondosus, B. tripartitus, B. pilosa, B. ferulaefolia) to 65-71% (B. bipinnatus, B. maximovicziana, B. cam-pylotheca); 38% with B. bitternata or no inhibition of parasite growth with B. parviflora. The latter contains no polyacetylene compounds whereas in B. bitternata three polyacetylenes were identified; and, all the others have from 6 to 14 polyacetylene compounds identified (Wat et al. 1979, Hoffmann & Hoelzl 1988, Christensen et al. 1990, Christensen & Lam 1991, Bauer et al. 1992, Redl et al. 1994). Thus, we believe that activity is related to the presence of polyacetylenes, possibly associated with flavonoids also present in B. pilosa (Brandão et al. 1997, 1998). In recent tests, two methoxylated flavone glycosides isolated from the roots of B. pilosa (Fig. 4) proved to be highly active in vitro (Table III). The activity we observed for extracts of Bidens spp. contrasts with previous results described in the literature using fenilheptatriyne, a phe-nylacetylene isolated from the leaves of Bidens collected in Africa (N'Dounga et al. 1983). The authors found little or no activity possibly because during fractionation or during storage of the fractions the active compounds were degraded. As it is now known, polyacetylenes degrade rather easily and lose activity (our unpublished data) as we observed when preparing them from the crude extracts of B. pilosa roots. The purified fraction developed a yellowish color overnight and after two days it became dark brown, even in the refrigerator (Brandão et al. 1997). "INDIAN BEER" Ampelozizyphus amazonicus A. amazonicus Ducke (Fam Rhamnaceae), a plant from the western Amazon, known as "Indian beer", is widely used there to prevent malaria rather than to treat the symptoms of the disease. According to riverine population, it has to be taken every day before bathing - one tablespoon of the dried ground roots in half a glass of water. The plant is thus used as a cold infusion of the roots, and is called "beer" from the intense foam it produces when the roots are shaken in water, due to its high saponin content (10% of the dry roots). "Indian beer" first came to our notice many years ago, through the Ministry of Health, in a written report by Dr Hipólito Paulino Filho (University of Araraquara, São Paulo) and others from the group of Professor Otto Gottlieb (University of São Paulo, now Fiocruz, Rio de Janeiro). We first tested the antimalarial activity of "Indian beer" using extracts from freshly ground roots kindly provided by Dr Paulino Filho. The aqueous and ethanolic extracts were tested against the blood stages in infected mice and chickens (Botelho et al. 1981/82). Purified fractions with or without saponins were also tested (Brandão 1991). No activity was found against the malarial blood stages in P. falciparum cultures in vitro, nor in mice infected with P. berghei, neither in chickens infected with P. gallinaceum. Surprisingly, the animals treated with Indian beer developed even higher parasitaemia, more severe anemia and died earlier then the non-treated malaria controls. This result was attributed to the saponin effect of the drug, which lysed the red blood cells, more fragile in the case of malaria infections. "Indian beer", unlike primaquine, had no activity against the sporogonic cycle in mosquitoes fed on malaria treated chickens. Thus it is presumably inactive also against P. vivax hypnozoites. It is known that all drugs that affect these late forms of sporozoite development in P. vivax, inhibit sporogony as well as proposed by Gwadz et al. (1983). We confirmed the ability of primaquine to inhibit the development of sporogony in Aedes fluviatilis mosquitoes fed on P. gallinaceum infected chickens previously treated with this drug; in contrast, "Indian beer" did not affect malaria sporogony (Carvalho et al.1992). It was frustrating to conclude that the widespread use of a plant in popular medicine seemed to be unfounded, like many other plants believed to be active against malaria, whose action could not be confirmed in the laboratory. More recently, fresh extracts and soluble fractions from new lots of "Indian beer", collected by our group in the Amazon region, tested against sporozoite were found to be active. Thus, it appears that this anti-sporozoite activity of "Indian beer" is the explanation of its prophylactic activity in human malaria, a hypothesis yet to be proven. It is not clear if it acts directly on the sporozoite infectivity or against the initial exoerythrocytic (EE) stages of sporozoite development. The experiments were performed by inoculating sporozoites of P. gallinaceum, freshly isolated from experimentally infected A. fluviatilis mosquitoes, into chickens previously treated with 200 ml/kg "Indian beer" orally, during 5 to 8 days. We found that the ethanolic extract reduced the tissue parasitism by 67%, comparable to primaquine (not shown) or to sulfadiazine (Table IV) which kills the EE forms (Ferrari 1997, Carvalho et al. 1997). Only the freshly prepared extracts were active against the sporozoites and/or the early exoerythrocytic parasites in the cerebral endothelial cells of chickens (Ferrari 1997), which roughly correspond to the liver stages in human malaria as they are the pre-erythrocytic forms. One goal should be to isolate the active molecule and/or to stabilize the ethanolic extracts shown to be active against the sporozoite induced infections. In the endemic areas of malaria, the fresh infusion of "Indian beer" is daily prepared and used to prevent human infections. Sporozoites, when injected into the vertebrate by the mosquito bite, have to reach the liver rapidly, where they enter the hepatocytes and develop. Once inside the hepatocytes, the sporozoites are likely to be more protected from drug action. Our present study seeks to confirm these experiments in mammalian malaria, using sporozoite induced infections in mice and monkeys, more complex models to work with in Brazil (Krettli 1994). Another important goal in our work is to clarify the mechanism by which this popular Amazonian antimalarial plant works, further studies are needed to confirm the activity in humans, naturally exposed to sporozoite infections. Direct surveys will be necessary among the riverine populations first localized by our collaborator and pioneering malarial ethnopharmacologist, Hipólito Paulino Filho, no longer among us (see also review in Krettli 1994, Carvalho et al. 1997). PROBLEMS AND PERPECTIVES Testing antimalarials has had an important by-product: the training of students and technicians to work on malaria chemotherapy models, to learn and maintain at regular basis the complete malaria cycle, including the sporogonic stages, to test the drugs against the schizogonic cycles, in vivo and in vitro, as well as in the mosquitoes, and to use scientific protocols for basic research. This training hopefully will permit new drugs to be developed in conjunction with local industry for the treatment of prevalent diseases, including new medicines against malaria. Such development, urgently needed, has immediately high costs, necessarily divided between Government, industry and international finance. At present a new type of interaction between basic research, industry and international corporations is developing in the tropical world. Research on antimalarial drugs is a typically multidisciplinary task involving student and senior research workers in botany, phytochemistry, parasitology, toxicology and medicine. Patent restrictions often limit immediate data publication pointing to the necessity for new rules adequate for product development and, at the same time, to students who need publications as part of their thesis requirements. It is noteworthy that under present law patents protect discoveries on plants and other biological material in North America but not in Brazil! The law needs re-exam in the light of research based on drugs from Brazilian plants to fight neglected diseases, a field unlikely to generate large profits, even under patent. The Integrated Program initiated in 1987 by the Ministry of Health Drug Agency - Ceme, and by the National Research Council of Brazil - CNPq, for the investigation of native medicinal plants, brought several chemical groups into contact with plants of popular use. The grounds for such research in Brazil were organized but many of the resulting data still lack validation. A definite tendency in the Ministry of Health and by State Health authorities to organize and regulate a popular use of medicinal plants to treat diseases has highlighted the shortcomings of teas and other formulations made from fresh plants, in which the identity, concentration and safety of active molecules are unknown. The structural identification and stabilization of these molecules will be the basis for the manufacture of new drugs suitably evaluated in pre-clinical trials and in controlled double blind clinical assays. ACKNOWLEDGMENTS To many students who tested antimalarial drugs, often an unrewarding task considering the bulk of negative results; to phytochemists from Brazilian Institutions, for providing plant extracts or molecules; to AJ Lapa and his secretariat for collecting and typing my conference (AUK) in the Congress of Medicinal Plants, Águas de Lindóia, SP, the basis of the present review; to B Gilbert for critical review of the manuscript; to Brenda Marshall, NIH-extramural, for editorial help, to Maria Inês O Mascarenhas and João Estabile (CPqRR-Fiocruz) for help with manuscript corrections. To the anonymous referee for many invaluable corrections and suggestions. REFERENCES
Copyright 2001 Instituto Oswaldo Cruz - Fiocruz. The following images related to this document are available:Photo images[oc01201t2.jpg] [oc01201f3.jpg] [oc01201f2.jpg] [oc01201t1.jpg] [oc01201f4.jpg] [oc01201t3.jpg] [oc01201f1.jpg] [oc01201t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}