
|
Memórias do Instituto Oswaldo Cruz
Fundação Oswaldo Cruz, Fiocruz
ISSN: 1678-8060 EISSN: 1678-8060
Vol. 97, Num. 1, 2002, pp. 47-49
|
Mem Inst Oswaldo Cruz, Rio de
Janeiro, Vol. 97(1) 2002, pp. 47-49
Neutralizing Antibodies to
Enterovirus 71 in Belém, Brazil
Maria de Lourdes C Gomes/+, Ceyla
Maria O de Castro**, Maria José C Oliveira*, Edson Elias da Silva**
Seção de Virologia, Instituto Evandro
Chagas, Funasa, Av. Almirante Barroso 492, 66090-000 Belém, PA, Brasil
*Fusam, Secretaria de Estado de Saúde, Recife, PE, Brasil **Instituto
Oswaldo Cruz-Fiocruz, Rio de Janeiro, RJ, Brasil
+Corresponding author. Fax:+55-91-214.2005. E-mail: lourdesgomes@iec.pa.gov.br
Received 16 March 2001
Accepted 10 September 2001
Code Number: oc02007
Non-polio enteroviruses (Coxsackievirus A,
Coxsackievirus B, Echovirus and EV 68-72) which belong to the enterovirus (EV)
genus, Picornaviridae
family, may be responsible for acute flaccid paralysis, aseptic meningitis,
myocarditis, hepatitis, pleurodinia, neonatal sepsis, hand, foot and mouth disease
(HFMD) even though 50-80% of infections are asymptomatic. EV 71 has been responsible
for outbreaks and epidemics of HFMD and acute neurologic disease justifying
its study in our country. The aim of this study was to detect neutralizing antibodies
(NtAb) to EV 71 in individuals up to 15 years of age living in Belém,
State of Pará, northern Brazil. Serum samples from 238 patients attending
the Virology Sector of Evandro Chagas Institute in Belém, Brazil, were
analyzed using microneutralization tests that included RD cells and BrCr strain.
Overall 40.8% (97/238) of tested samples had NtAb to EV 71. Regarding the distribution
per age group, 85.2% (92/108) of patients aged 0-3 years had no NtAb to this
virus and 69.2% of those 12 to15 years of age were seropositive. These results
confirm that EV 71 infection occurs in the city of Belém; and that a
high rate of individuals in this study were infected aged 3 years and over and,
when aged 15 years nearly 70% had EV 71 NtAb.
Key words: enterovirus 71- neutralizing antibodies
to EV 71 - seroepidemiology study - Belém - Brazil
At the beginning of this century, motor deficiency
cases could be related to pathogens such as viruses and particularly to polioviruses,
which belong to the enterovirus (EV) genus, Picornaviridae family. Besides
the poliovirus (3 serotypes), EV includes Coxsackievirus A (23 serotypes: types
1-17, 19-22 and 24), Coxsackievirus B (6 serotypes), Echovirus (30 serotypes):
1-7, 9, 11-27, 29-33), and EV 68-72 (Wiedbrank & Johnston 1993).
Enteroviruses are non-enveloped small viruses
(20-30 nm) of icosahedral symmetry. Their RNA genomes have 7.5 kb, positive
sense and single strand. They are responsible for an extensive variety of diseases,
although 50 to 80% of the infections are asymptomatic. They cause hepatitis,
pleurodinia, stomatitis and neonatal sepsis in a significant number of patients
every year. In developing countries, the poliovirus is clinically the most significant
member of the genus EV causing paralysis diseases in every 4 out of 1,000 children
in school age. The non-polio enteroviruses (NPEV) are the main responsible for
aseptic meningitis, myocarditis and nonspecific febrile exanthematous illnesses.
Approximately 75% of infections by EV occur in children under 15 years of age
and the attack rates are highest in children under 1 year of age (Wiedbrank
& Johnston 1993).
EV 71, one of the last NPEV studied, was described
for the first time by NJ Schimidt et al. (da Silva et al. 1990) in 1974, in
California, associated with cases of the central nervous system (CNS) diseases.
In the same year Kennett et al. (1974) mentioned the occurrence in Melbourne,
Australia, of cases of aseptic meningitis, cutaneous eruption, acute respiratory
tract infections and infective polyneuritis caused by EV 71. In 1975, an epidemic
was observed in Bulgaria with clinical symptoms of poliomyelitis, encephalitis,
encefalomyocarditis and aseptic meningitis. Ninety-two strains of EV 71 were
isolated from the 65 cases with the same symptomatology of the poliomyelitis,
including 37 strains from brain and medulla, 1 from cerebrospinal fluid, 10
from mesenterial lymph nodes and tonsils and 44 from feces (Chumakov et al.
1979). An outbreak of infections caused by EV 71 occurred in Australia during
the winter of 1986. Of the 114 studied patients, 65 were hospitalized and 33
frequently had CNS involvement associated to severe symptoms (Gilbert et al.
1988). During an outbreak of hand, foot and mouth disease (HFMD) in Malaysia,
in 1997, 4 children developed cardiopulmonary collapse and neurological problems.
All the children received cardiopulmonary resuscitation but died. Postmortem
studies showed infection by EV 71, with extensive damage to the medulla and
pons (Lum et al. 1988). More recently the EV 71 was responsible for an epidemic
occurred in Taiwan. Most of the patients had HFMD with or without complications.
Many enteroviruses were isolated from the 238 cases, approximately half of them
were EV 71 (Wang et al. 1998). In Brazil the first evidence of infections by
EV 71 was mentioned by da Silva et al. (1990); these authors studied cases of
acute flaccid paralysis (AFP) and finding neutralizing antibodies (NtAb) for
EV 71 in 32.1% of serum samples. In another study developed by da Silva et al.
(1996) positive IgM to EV 71 was detected in 20 (21%) of 92 children living
in different areas of Brazil that presented clinical symptoms of AFP over a
3 year-old period (1988 to 1990). Takimoto et al. (1998) detected positivity
for EV 71 in 5.6% of the 426 samples of children's feces with symptoms of acute
neurological disease (AND), residents in the State of São Paulo and in
the city of Brasília. Despite the significant variability of clinical
and epidemic manifestations, there is close antigenic similarity among strains
of EV 71 isolated in different countries (da Silva et al. 1990), justifying
its study in several aspects including seropreva-lence. On this subject Hagiwara
et al. (1979) in the 70s showed interesting results including reference to circulation
of EV 71 in Japan in 1966. It is important to mention that the presence of this
virus in the community is concerning, considering the evaluation of the poliomyelitis
control program (Blal et al. 1998 ).
The aim of this work was to detect NtAb to the
EV 71 in serum samples from patients up to 15 years of age living in the city
of Belém, Brazil.
MATERIALS
AND METHODS
Patients - Serum samples from 238 patients
of both sexes aged up to 15 years and residents in the city of Belém,
were included in this study with symptoms of fever and exanthem. Patients received
care from the Virology Section of the Evandro Chagas Institute during the year
of 1998.
Cell culture - RD cell (rabdomiosarcoma
of human origin) was used, and maintained in Eagle's MEM (Minimum Essential
Medium) with Earle's salts, without sodium bicarbonate and without phenol red.
The preparation of this medium was as follows: MEM powder was added with (9.7
g, sodium bicarbonate 1.5 g , fetal bovine serum 100 ml, L-glutamine 200 mM
2 ml, HEPES 1 M 10 ml, penicillin 100,000 U/ml, and streptomycin 100,000 µg/ml,
1 ml of each) in 1,000 ml of distilled and purified water. This mixture was
filtered in membranes of 0.22 µm, distributed in small volumes and maintained
at 4°C. The RD cells were maintained weekly using Trypsin 0.25% plus EDTA.
Virus - An aliquot of EV 71, BrCr strain,
provided by EE da Silva, was inoculated in RD cells to obtain a large volume.
When the cellular layer presented 75% of cytopathic effect, the cultivation
was frozen and thawed three times, centrifuged at 3,000 rpm for 30 min; the
supernatant was distributed in aliquots of 500 µl and frozen at -20°C.
Neutralization microtechnique - Aliquots
of 100 µl of serum were separated, inactivated at 56°C for 30 min and
diluted 1:8 in Eagle's MEM (prepared equal to the growth medium except in the
bovine serum concentration that decreased to 2% and the increase of 0.06% of
anfothericin B 5,000 µg/ml), which was used as diluent of the test. The
protocol utilized in this test was the same used for polioviruses (WHO 1996)
with some modifications. Initially 50 µl of the diluent was put into all
wells of the microplate (polystyrene, 96 flat bottom wells) except for the first
row, then 50 µl of 1:8 dilution serum was put in the first and second
rows. With the aid of the multichannel pipette, serum samples were diluted starting
from the second row, removing 50 µl and placing it into the third row
and so forth until the last dilution. In the following stage, 50 ml of virus
contends the challenge dose (100 TCD50 with variations from 31.5 to 315) was
added. Two incubation periods were used: 2 h at 37°C in CO2 incubator,
and overnight at 4°C. The next day 100 µl of the suspension of RD cells
with 3 days of growth was added, in the concentration of 2x105 cells/ml.
They were maintained at 35°C in CO2 incubator. Microscopic observation
was made on the 5th day.
RESULTS
In the analysis of 238 serum samples it was verified
that the largest percentage of samples tested against EV 71 were located in
the age group up to 3 years, with 45.4%, followed by the 4 to 7 years-old with
24.4%. The rest were divided into the 8 to 11 years-old (19.3%) and 12 to 15
years-old (10.9%) age groups. In terms of gender, 54.2% were female and 45.8%
male.
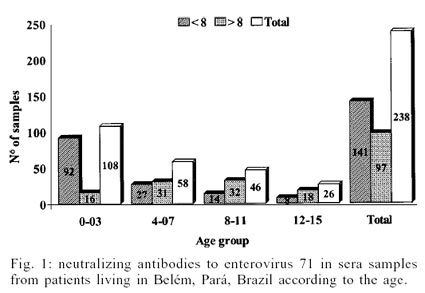
Fig. 1 relates
the levels of antibodies less (<) than 1:8 and higher or equal to (³)
1:8, with the patients' age group. It was observed that in 59.2% the level of
antibodies was < 1:8 and in 40.8% ³ 1:8.
In the age group from 0 to 3 years which included 108 cases, 85.2% showed a
level of < 1: 8 while 14.8% ³1:8. In the
4 to 7 years-old group, an inversion of percentage was noted because in the
dilution ³ 1: 8, the percentage increased to
53.4% while at < 1:8 it decreased to 46.6%. The 8 to 11 and 12 to 15 years-old
groups showed a pattern similar to the previous one.
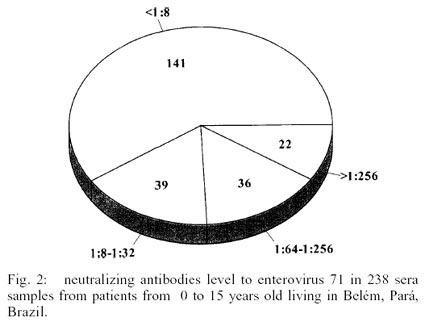
Fig. 2 shows
the four groups of levels of NtAb detected in the samples of these patients.
Of the 238 samples tested, 141 (59.2%) presented level of < 1: 8.The two
following groups 1:8-1:32 and 1:64-1:256 contained 39 (16.4%) and 36 (15.1%)
samples respectively. The last group, > 1: 256 included 22 (9.2%) samples.
DISCUSSION
Studies involving detection of NtAb to EV 71
are scarce and when existent they are related to the cases of HFMD, AND in general,
and AFP in particular. As the main objective of this work was to verify the
seroprevalence in a group of individuals with less than 15 years of age presenting
different symptomatology, it was difficult to discuss our results.
Hagiwara et al. (1979) analyzing 137 samples
of healthy children from 0 to 10 years of age, living in the city of Kawasaki,
in Japan detected 6.6% with NtAb to EV 71. In our study the percentage corresponding
to the patients up to 11 years of age was 37.3%. The use of different cells
lines, Cynomolgus monkey cell line (CMK1-S1) in the Japanese study and RD in
our study could have influenced these results. It is also possible that in the
period in which the Japanese evaluation was done, circulation of EV 71 was extremely
low and perhaps restricted to a determined country. In Brazil studies involving
EV 71 were carried out by da Silva et al. (1990) and Takimoto et al. (1998)
both relating that this viruses to motor disorder occurred in the states of
Bahia, Goiás, Piauí, São Paulo and Federal District, different
from our study that involved patients with fever and exanthem. These authors
detected positivity to EV 71 in 32.1% (9/28) and 5.6% (24/426) of the cases
respectively. Our results show a percentage of 40.8% (97/238). It is evident
that a great number of people were infected by EV 71 in Belém in contrast
to the low number of individuals infected in São Paulo. Our percentage
of infection is closer to the percentage found by da Silva et al. (1990) in
the other localities. In relation to clinical symptoms the patients studied
by Takimoto et al. (1998) and da Silva et al. (1990) presented disease with
motor involvement while our patients presented fever and exanthem. Probably
the strain of EV 71 that has circulated in Belém is genetically different
from the strain that has circulated in the localities studied by that authors.
According to our results the infection by EV 71 in Belém occurred with
great frequency after 3 years of age considering that the individuals in the
age group 0-3 years with NtAb > 1:8 was 14.8% (16/238). Another point is
that a large number of individuals when reaching the age of 15 years posses
NtAb to EV 71 considering the percentage of 69.2% (18/26) detected. In relation
to the children with AND studied by Takimoto et al. (1998) the majority was
infected later because until 5 years of age the percentage of individuals infected
was 7.3% (17/231).
Although the importance of EV 71 has already
been defined, more studies will be necessary in order to increase the knowledge
on the several aspects related to this virus in Brazil. The data obtained in
this study will be used for comparison with other studies in different localities
of Brazil where this virus can be associated to other clinical disorders.
ACKNOWLEDGEMENTS
To Dr Yvone Gabbay for critically reviewing this
manuscript.
REFERENCES
- Blal CA, Figueiredo HG, Silveira EA, Souza
MC, Morais LM, da Silva EE 1998. Laboratory diagnosis of the enterovirus 71
( EV 71) responsible for cases of acute flaccid paralysis in Brazil. Virus
Rev Res 3 (Suppl. 1): 99.
- Chumakov M, Voroshilova M, Shindarov L, Lavrova
I, Gracheva L, Koroleva G, Vasilenko S, Brodvarova I, Nikolova M, Gyurova
S, Gacheva M, Mitov G, Ninov N, Tsylka E, Robinson I, Frolova M, Bashkirtsev
V, Martiyanova L, Rodin V 1979. Enterovirus 71 isolated from cases of epidemic
poliomyelitis-like disease in Bulgaria. Arch Virol 60: 329-340.
- da Silva EE, Fillipis AM, Schatzmayr HG, Cortes
LC 1990. Evidence of enterovirus 71 infection in Brazil. Mem Inst Oswaldo
Cruz 85: 131-132.
- da Silva EE, Winkler MT, Pallansch MA 1996.
Role of enterovirus 71 in acute flaccid paralysis after the eradication of
poliovirus in Brazil. Emerg Infect Dis 2: 231-233.
- Gilbert GL, Dickson KE, Waters MJ, Kennett
ML, Lands SA, Sneddon M 1988. Outbreak of enterovirus 71 infection in Victoria,
Australia, with a high incidence of neurologic involvement. Pediatr Infect
Dis J 7: 484-488.
- Hagiwara A, Tagaya I, Komatsu T 1979. Seroepidemiology
of enterovirus 71 among healthy children near Tokyo. Microbiol Immunol
23:121-124.
- Kennett ML, Birch CJ, Lewis FA, Yung AP, Locarnini
SA, Gust ID 1974. Enterovirus 71 infection in Melbourne. Bull WHO 51:
609-615.
- Lum CS, Wong KT, Lam SK, Chua KB, Gok AY,
Lim WL, Ong BB, Paul G, AbuBakar S, Lambert M 1998. Fatal enterovirus 71 encephalomyelitis.
J Pediatr 133: 795-798.
- Takimoto S, Waldman EA, Moreira RC, Kok F,
Pinheiro FP, Saes SG, Hatch M, Souza DFC, Carmona RCC, Shout D, Moraes JC,
Costa AM 1998. Enterovirus 71 infection and acute neurological disease among
children in Brazil (1988-1990). Trans R Soc Trop Med Hyg 92:
25-28.
- Wang J-R, Tsai H-P, Chen P-F, Lai Y-J, Yan
J-J, Kiang D, Lin K-H, Lin C-C, Su I-J 1998. An outbreat of enterovirus 71
infection in Taiwan, 1998. II. Laboratory diagnosis and genetic analysis.
J Clin Virol 17: 91-99.
- WHO-World Heath Organization 1996. Manual
for the Virological Investigation of Polio,WHO, Geneve, 42 pp.
- Wiedbrauk DL, Johnston SLG 1993. Enteroviruses.
In DL Wiedbrauk, SLG Johnston (eds), Manual of Clinical Virology, Raven
Press, New York, p. 92-97.
© 2002
Instituto Oswaldo Cruz - Fiocruz
The following images related to this document are available:
Photo images
[oc02007f1.jpg]
[oc02007f2.jpg]
|

{kind=link}
{kind=link}