
|
Memórias do Instituto Oswaldo Cruz
Fundação Oswaldo Cruz, Fiocruz
ISSN: 1678-8060 EISSN: 1678-8060
Vol. 97, Num. 1, 2002, pp. 105-107
|
Mem Inst Oswaldo Cruz, Rio de
Janeiro, Vol. 97(1) 2002, pp. 105-107
Detection of Hepatitis B Virus
Antigens in Paraffin-embedded Liver Specimens from the Amazon Region, Brazil
SRR Simonetti, HG Schatzmayr, OM Barth+,
JP Simonetti
Departamento de Virologia, Instituto Oswaldo
Cruz-Fiocruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil
+Corresponding author. Fax: +55-21-2270.6397. E-mail: barth@ioc.fiocruz.br
This work received financial support from
the Conselho Nacional de Desenvolvimento Científico e Tecnológico
(CNPq), Brazil.
Received 3 May 2001
Accepted 5 September 2001
Code Number: oc02019
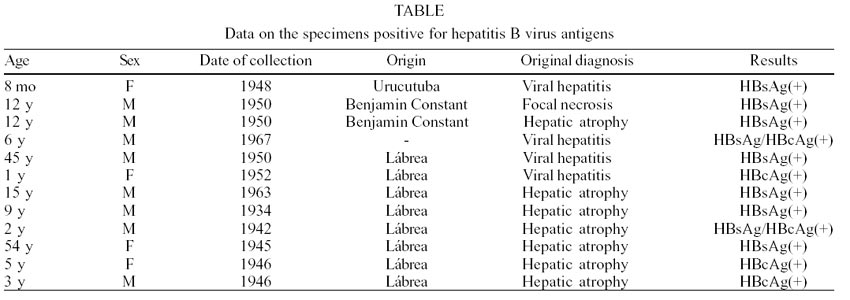
Hepatic viscerotomy of paraffin-preserved
old specimens, collected in the period from 1934 to 1967, were analyzed by immunohistochemical
assays to detect hepatitis B, hepatitis D, dengue and yellow fever virus antigens.
The material belongs to the Yellow Fever Collection, Department of Pathology,
Instituto Oswaldo Cruz, Rio de Janeiro, Brazil and the cases were diagnosed
at that time according to clinical aspects and histopathological findings reporting
viral hepatitis, yellow fever, focal necrosis and hepatic atrophy. From the
79 specimens, 69 were collected at the Labrea Region and the other 10 in different
other localities in the Amazon Region. The five micra thick histological slices
were analyzed for the presence of hepatitis B surface antigen (HBsAg) and hepatitis
B core antigen (HBcAg) by immunoperoxidase technique. An immunofluorescence
assay was applied to the detection of hepatitis D, yellow fever and dengue virus
antigens. Nine (11.4%) histological samples were HBsAg reactive and 5 (6.3%)
were HBcAg reactive. The oldest reactive sample was from 1934. Viral antigens
related to the other pathologies were not detected in this study. Our results
confirm that the methodology described may be used to elucidate the aetiology
of hepatitis diseases even after a long time of conservation of the specimens.
Key words: hepatitis B virus - human liver -
Amazon - Brazil
According to the World Health Organization, hepatitis
B virus (HBV) carriers account for 5% of the world population. These potential
infection transmitter individuals can evolve from the asymptomatic condition
to a severe hepatic damage and even hepatocellular carcinoma. A similar HBV
epidemiological distribution is observed for hepatitis D virus (HDV) that shares
the obligatory association to HBV for its replication (Smedile et al. 1981).
Frequently related to HBV chronic carriers and less frequently to the acute
disease forms (Colombo et al. 1983, Rizzetto et al. 1983), HDV antigen was identified
by immunohistochemical assays in liver cell nuclei of patients with chronic
persistent or chronic active hepatitis, hepatitis B surface antigens (HBsAg-positive)
(Rizzetto et al. 1977). In South America HDV infection was first observed in
Venezuela as a severe and fulminant attack among Yucpa indians (Purcell &
Gerin 1983) and in Colombia where 60% of the individuals studied were simultaneously
HBV and HDV reactive (Ljunggren et al. 1984). In Brazil, the Amazon Region endemicity
for both viruses is well known (Figueiredo Mendes et al. 1984, Fonseca et al.
1986, Simonetti et al. 1986) showing high prevalence pattern compared to the
other parts of the world (Purcell & Gerin 1983, Nordenfelt et al. 1983,
Fonseca et al. 1988). This region is also endemic for yellow fever and it is
thought whether another human hepatitis viruses had been introduced in this
area by human serum present in vaccines against yellow fever, since there are
observations on the occurrence of icterus in England and in Brazil, following
vaccination against yellow fever in the 1930s and 1940s decades (Findlay &
Mac Callum 1937, 1938, Soper & Smith 1938, Fox et al. 1942). We included
the dengue virus antigen research in this study, once the same pathological
liver findings are observed in yellow fever and haemorrhagic dengue, such as
hepatomegaly, focal visceral haemorrhages, focal necrosis, sinusoidal acidophilic
bodies, Kupffer cell hypertrophy and portal tract mononuclear cell infiltration.
To observe the simultaneous HBV and HDV antigen
frequency and to detect yellow fever and dengue viral antigens in histological
sections we studied 79 hepatic samples by immunohistochemical assays. Hepatic
viscerotomy samples belong to the Yellow Fever Collection (Department of Pathology,
Instituto Oswaldo Cruz, Brazil) created in the 1930s decade from an agreement
between Brazilian Government and the Rockefeller Foundation International Division
to study yellow fever in Brazil.
MATERIALS AND
METHODS
Material - Seventy-nine paraffin-embedded
hepatic samples collected from 1934 to 1967 were analyzed. Sixty-nine samples
were from the Labrea Region, State of Amazonas and ten random samples were from
other different localities in the same state. The cases were diagnosed at that
time as viral hepatitis, yellow fever, focal necrosis or hepatic atrophy according
to clinical aspects and histopathological findings.
Methods - Four or five micra thick paraffin-embedded
histological sections were prepared for hepatitis B, hepatitis D, yellow fever
and dengue virus antigen detection by immunoperoxidase or immunofluorescence
techniques. HBsAg and hepatitis B core antigens (HBcAg) were detected by the
immunoperoxi-dase assay (Immuno Tag S - Immunon-Lipshaw Corporation). Paraffin
sections were deparaffinated and treated with 90% and 85% ethyl alcohol solutions
followed by 10% ammonium hydroxide solution. To block endogenous peroxidase,
sections were incubated with 3 to 10% hydrogen peroxidase solution for 5 min.
Sections were then incubated with peroxidase/anti-peroxidase conjugate, stained
with hematoxylin solution (1 min) and treated with 0.2% ammonium hydroxide solution.
The reaction colour was developed after 3-amino-9-ethylcarbazole substrate addition.
Positive HBsAg and HBcAg controls were included for every batch. HDAg was detected
by the immunofluorescence assay as follows: 5 µm thick paraffin-embedded
sections were deparaffinated, rehydrated and digested with 0.1% protease solution
(type XXVII Sigma) in Tris-HCl 0.5M pH 7.4 for 2 h at 37ºC or 0.05% trypsin
(Difco) in phosphate buffered saline pH 7.4 for 10 min at 37ºC. Digested
sections were incubated at room temperature for 30 min with FITC-anti HD conjugate
diluted 1:100 in PBS pH 7.4. Yellow fever and dengue virus antigens were tested
by immunofluorescence (Huang et al. 1976, Walker & Cain 1978, Schatzmayr
et al. 1984, Barth et al. 1988): 4 µm thick paraffin sections were deparaffinated,
rehydrated and digested with 0.1% trypsin with 0.1% CaCl2 solution
in PBS pH 7.8 for 2 h at 37ºC. Digested sections were incubated at 37ºC
for 30 min with FITC-conjugated yellow fever positive simian serum diluted at
1:20 in PBS pH 7.2. Flavivirus hyperimmune ascitic fluid obtained from mouse
was used to detect dengue virus antigen. After washing sections were mounted
with buffered glycerol and examined at the UV microscope. Four controls were
used for yellow fever virus detection: not infected Vero cells, yellow fever
virus (17D strain)-infected Vero cells, not infected liver cells and HBV-infected
liver cells. Aedes albopictus C6/36 infected cell line was included as
positive control for dengue virus detection.
RESULTS
Nine (11.4%) of 79 hepatic samples were HBsAg-reactive
and 5 (6.3%) were HBcAg-reactive by immunoperoxi-dase assay (2 of them showed
reactivity for both viral markers). HDAg was detected in none of these reactive
samples. HBsAg and HBcAg were more frequently seen in samples from people at
lower ages since in both groups examined (male and female) we had a higher number
of samples from persons under 21 years old. Two samples showing simultaneous
HBsAg and HBcAg reactivity were from boys agged 2 and 6 years. Chronological
distribution of viral markers detected in this study showed that old preserved-paraffin
liver samples are still suitable for viral markers detection by immunoperoxidase
assay. The results are shown in the Table.
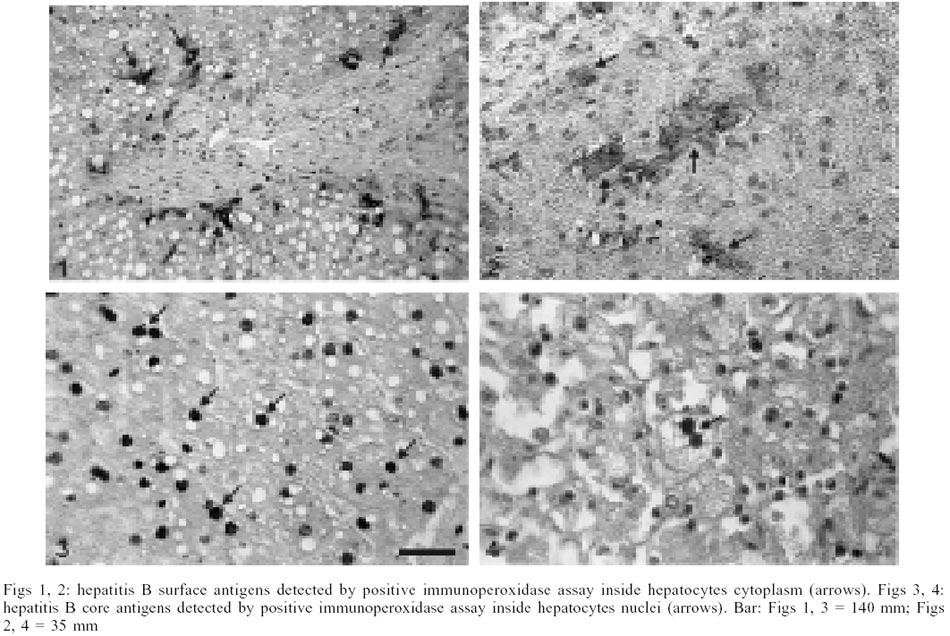
An exclusive cytoplasmic HBsAg localization and
an exclusive nuclear HBcAg localization were observed by immunoperoxidase assay.
The results are shown in Figs 1-4.
Yellow fever and dengue virus antigens were seen
in none of the 79 hepatic samples by immunofluorescence assay.
DISCUSSION
The Labrea Region, State of Amazonas, shows a
high HBV endemical level (Figueiredo Mendes et al. 1984, Fonseca et al. 1988);
this was an important point in sample selection and could have influence on
the uneven age range distribution observed. Hepatitis B virus antigen detection
in the liver tissue samples by immunohistochemical assays showed a cytoplasmic
HBsAg and a nuclear HBcAg localization.
Only the HBsAg-reactive (9 of 79) and HBcAg-reactive
(5 of 79) samples were analyzed for the presence of HDAg. None of them showed
reactivity. The possible explanations for this are (1) HDV is mainly found in
young adults and 71.3% of people analyzed in our study were children under 14
years old (Fonseca et al. 1988); (2) the immunofluorescence method had low sensitivity
that could not detect HDV antigen in low level concentration samples; and (3)
the more recent HDV introduction in this region, which would be subsequent to
the analysis period of the samples (Fonseca et al. 1986, 1988, Simonetti et
al. 1986).
The retrospective analysis evidenced HBsAg preservation
in old histological samples. The oldest one, from 1934, was from a 9 year old
boy from Labrea Region, Amazonas, with a negative yellow fever diagnosis.
All the 79 samples were analyzed for dengue and
yellow fever virus antigen detection. The results were negative. This could
be due to the low sensitivity of the method, as discussed for HDV (Fonseca et
al. 1988). Alternatively, other viruses causing acute liver inflamation and
necrosis, determining similar hepatic lesions to those described, or non-viral
fatal infections such as malaria and leptospirosis, could be considered aetiological
agents.
Our results confirm that the methodology described
may be used to elucidate the aetiology of hepatitis diseases even after long
time of conservation of the specimens. Retrospective studies of viral infection
of the liver (Schatzmayr et al. 1984) were used in order to acquire a better
knowledge of the natural history of these diseases and to may compare the data
obtained with the actual distribution of hepatitis in the Amazon region.
ACKNOWLEDGMENTS
To Ms Itália B Kerr, Department of Pathology,
Instituto Oswaldo Cruz, for delivery of specimens and related data. To Ms Ângela
T Pinhão, Department of Virology, Instituto Oswaldo Cruz and to Dr Carlos
Alberto Basílio, Pathology Service, Gafrée Guinle University Hospital,
Rio de Janeiro, for technical assistance.
REFERENCES
- Barth OM, Majerowicz S, Menasce LP, Schatzmayr
HG 1988. Detection of viral infection by immunofluorescence in formalin-fixed
tissues, pretreated with trypsin. Mem Inst Oswaldo Cruz 83: 207-212.
- Colombo M, Cambieri R, Rumi MG, Rouchi G,
Ninno E, Franchis R 1983. Long-term delta superinfection in hepatitis B surface
antigen carriers and its relationship to the course of chronic hepatitis.
Gastroenterology 85: 235-239.
- Figueiredo Mendes T, Simonetti JP, Fonseca
JCF, Simonetti SRR, Pittella AM, Schatzmayr HG, Ferreira LCL, Santos IM, Mexas
PPF, Herbert BA 1984. O impacto da hepatite delta. Moderna Hepatologia
(Boletim do Serviço de Hepatologia da Santa Casa do Rio de Janeiro)
9: 16-22.
- Findlay GM, Mac Callum FO 1937. Note on acute
hepatitis and yellow fever immunization. Trans R Soc Trop Med Hyg 31:
297-308.
- Findlay GM, Mac Callum FO 1938. Hepatitis
and jaundice associated with immunization against certain virus diseases.
Proc R Soc Med 31: 799-806.
- Fonseca JCF, Simonetti SRR, Simonetti JP 1986.
Hepatite por vírus delta. In O Borba Junior, Gastroenterologia,
Medsi, Rio de Janeiro, p. 229-234.
- Fonseca JCF, Simonetti SRR, Schatzmayr HG,
Castejón MJ, Cesário ALO, Simonetti JP 1988. Prevalence of infection
with hepatitis delta virus (HDV) among carriers of hepatitis B surface antigen
in Amazonas State, Brazil. Trans R Soc Trop Med Hyg 82: 469-471.
- Fox JP, Manso C, Penna HA, Pará M 1942.
Observations on the occurrence of icterus in Brazil following vaccination
against yellow fever. Am J Hyg 36: 68-116.
- Huang S, Minassian H, More JD 1976. Application
of immunofluorescence staining on paraffin sections improved by trypsin digestion.
Lab Invest 35: 383-390.
- Ljunggren K, Patarroyo ME, Engle R, Purcell
RH, Gerin JL 1984. Viral hepatitis and delta agent in Colombia. In GN Vyas,
JL Dienstag, JH Hoofnagle (eds), Viral Hepatitis and Liver Disease,
Grune & Stratton, Orlando, p. 616.
- Nordenfelt E, Hansonn BG, Al Nakib B 1983.
Frequency of delta agent infections in Kuwait. J Infect Dis 143:
768-769.
- Purcell RH, Gerin JL 1983. Epidemiology of
the delta agent: an introduction. In M Rizzetto, G Verme, F Bonino (eds),
Viral Hepatitis and Delta Infection, Alan R Liss, New York. p. 113-119.
- Rizzetto M, Canese MG, Arico S, Crivelli O,
Trepo C, Bonino F, Verme G 1977. Immunofluorescence detection of new antigen-antibody
system (delta/anti-delta) associated to hepatitis B virus in liver and in
serum of HBsAg carriers. Gut 18: 997-1003.
- Rizzetto M, Verme G, Recchia S, Bonino F,
Farci P, Arico S, Calzia R, Picciotto A, Colombo M, Popper H 1983. Chronic
hepatitis in carriers of hepatitis B surface antigen with intrahepatic expression
of delta antigen. Ann Intern Med 98: 437-441.
- Schatzmayr HG, Barth OM, Alencar AA 1984.
Demonstração por imunofluorescência direta de antígenos
do vírus da febre amarela em tecido hepático pré-tratado
com tripsina. Mem Inst Oswaldo Cruz 79: 93-99.
- Simonetti SRR, Fonseca JCF, Simonetti JP 1986.
Vírus da hepatite delta. In O Borba Junior, Gastroenterologia,
Medsi, Rio de Janeiro. p. 219-227.
- Smedile A, Dentico P, Zanetti A, Sagnelli
E, Nordenfelt E, Actis GC, Rizzetto M 1981. Infection with the delta agent
in chronic HBsAg carriers. Gastroenterology 81: 992-997.
- Soper FL, Smith HH 1938. Yellow fever vaccination
with cultivated virus and immune and hyperimmune serum. Am J Trop Med 18:
111-134.
- Walker DH, Cain BGA 1978. A method for specific
diagnosis of Rocky Mountain spotted fever on fixed paraffin-embbeded tissue
by immunofluorescence. J Infect Dis 137: 206-209.
© 2002
Instituto Oswaldo Cruz - Fiocruz
The following images related to this document are available:
Photo images
[oc02019t1.jpg]
[oc02019f1-4.jpg]
|

{kind=link}
{kind=link}