 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(3) 2002, pp. 289-295 Integrate Study of a Bolivian Population Infected by Trypanosoma cruzi, the Agent of Chagas Disease Simone Frédérique Brenière/+, Marie France Bosseno, François Noireau*, Nina Yacsik**, Pascale Liegeard***, Christine Aznar****, Mireille Hontebeyrie***
Institut de Recherche pour le Développement
(IRD), UR 08 Pathogénie des Trypanosomatidae, 911 Av. Agropolis, BP 5045,
34032 Montpellier Cedex 1, France *Laboratório Nacional e Internacional
de Referência em Taxonomia de Triatomíneos, Departamento de Entomologia,
Instituto Oswaldo Cruz-Fiocruz, Rio de Janeiro, RJ, Brasil **Instituto Boliviano
de Biología de Altura, La Paz, Bolivia ***Laboratoire d'Immunopathogenèse,
Département d'Immunologie, Institut Pasteur, France ****UFR de Médecine,
Université des Antilles et de la Guadeloupe, Cayenne, Guyane Française
This work was supported by a grant of World Health Organization Special Program for Research and Training in Tropical Disease (no. 910273). Received 27 April 2001 Code Number: oc02056
A cross section of a human population (501 individuals) selected at random, and living in a Bolivian community, highly endemic for Chagas disease, was investigated combining together clinical, parasitological and molecular approaches. Conventional serology and polymerase chain reaction (PCR) indicated an active transmission of the infection, a high seroprevalence (43.3%) ranging from around 12% in < 5 years to 94.7% in > 45 years, and a high sensitivity (83.8%) and specificity of PCR. Abnormal ECG tracing was predominant in chagasic patients and was already present among individuals younger than 13 years. SAPA (shed acute phase antigen) recombinant protein and the synthetic peptide R-13 were used as antigens in ELISA tests. The reactivity of SAPA was strongly associated to Trypanosoma cruzi infection and independent of the age of the patients but was not suitable neither for universal serodiagnosis nor for discrimination of specific phases of Chagas infection. Anti-R-13 response was observed in 27.5% only in chagasic patients. Moreover, anti-R13 reactivity was associated with early infection and not to cardiac pathology. This result questioned previous studies, which considered the anti-R-13 response as a marker of chronic Chagas heart disease. The major clonets 20 and 39 (belonging to Trypanosoma cruzi I and T. cruzi II respectively) which circulate in equal proportions in vectors of the studied area, were identified in patients' blood by PCR. Clonet 39 was selected over clonet 20 in the circulation whatever the age of the patient. The only factor related to strain detected in patients' blood, was the anti-R-13 reactivity: 37% of the patients infected by clonet 39 (94 cases) had anti-R13 antibodies contrasting with only 6% of the patients without clonet 39 (16 cases).
Key words: Chagas disease - recombinant proteins - polymerase chain reaction - clones - Bolivia Chagas disease is an endemic infection affecting many Latin American countries. Bolivia is considered one of the most endemic countries. The endemic area covers 80% of the country and, in 1985 more than one million people were infected (WHO 1991). The vectorial transmission of Trypanosoma cruzi, the agent of the disease, is mainly assured by Triatoma infestans which presents a T. cruzi infection rate of around 30% (WHO 1991). The vector control program is not yet expanded over all the country and, due to the large chagasic population, congenital transmission and transmission by blood transfusion are very abundant too (Azogue et al. 1985, Azogue & Darras 1995). High seroprevalences reported in blood donors indicate the magnitude of the human infection even in the towns outside the endemic regions (Carrasco et al. 1990, Landivar et al. 1992). The rural population has been considered as the main population at risk of infection, however, it was recently shown that vectorial transmission is occurring in suburbs of the main cities too (Revollo et al. 1997, Albarracin-Veizaga et al. 1999). Moreover, cardiac morbidity as well as digestive alterations remain important (Weinke et al. 1988, Brenière et al. 1989, Pless et al. 1992). Recent developments in molecular biology applied to Chagas disease proposed new tools for a better knowledge of the natural human infection. PCR is proposed for sensitive detection of parasites in human blood (Moser et al. 1989, Avila et al. 1993, Wincker et al. 1997, Russomando et al. 1998). Several recombinant proteins allow specific and sensitive detection of antibodies directed against T. cruzi. Recombinant proteins have been proposed as stage or pathological specific markers while others should be relevant for cure criteria (Affranchino et al. 1989, Levin et al. 1989, 1991, Mesri et al. 1990, Aznar et al. 1995, Gomes 1997, Guevara et al. 1997). Genetic variability of T. cruzi is now well documented. This parasite is composed of natural clones which present high genetic differences and recent studies demonstrate the existence of two principal lineage; regarding the nomenclature, and in agreement between scientists, two groups are now named, T. cruzi I and T. cruzi II (Tibayrenc 1995, Luquetti et al. 1999). In Bolivia, two major distinct monophyletic groups of clones have been identified in the domestic cycle and, they belong to T. cruzi I and T. cruzi II respectively (Brenière et al. 1998). These groups named clonet 20 and 39 can be detected directly in blood by PCR and identified by hybridization with specific kDNA probes (Brenière et al. 1998). We report here a transversal study of a cross section of an entire human population living in a highly endemic area in Bolivia (Cochabamba Department), selected at random, in order to determine the magnitude of the human infection combining together clinical, parasitological and molecular approaches including the determination of the T. cruzi clones. Each parameter was analyzed according to age and sex, and their relationships studied. The usefulness of each molecular tool was also examined and discussed. MATERIALS AND METHODS
Studied area and patients - The 501 individuals examined were children, teenagers and adults all free of treatment and living in the village of Mizque (altitude 1,970 m) located in a highly endemic region for Chagas disease in Bolivia (Cochabamba Department). T. infestans was the only triatomine species collected in 100% of the dwellings and its T. cruzi infection rate was around 60%. In this area, insect control program had been implemented after the study. The community had 3,850 inhabitants. Blood samples were collected during 1994 and 1995 and the age of the patients ranged from 1 to 83 years old. Children and teenagers were mainly from elementary school and college and a written consent was obtained from parents. The adults were volunteers, born and residents of Mizque. The study included 281 children from whom serological and parasitological results were previously reported (Wincker et al. 1997). Interpretation of the ECG tracings - The electrocardiographic test (ECG) was applied among 232 individuals selected at random from the 501 studied including 123 chagasic patients. ECGs were recorded in 12 standard derivations using a portable Hewlett Packard electrocardiograph. Two physician doctors coded each tracing (without serological information of the cases) according to the classification previously proposed and discrepancies were resolved by mutual agreement (Maguire et al. 1982). The ECG's showing atrioventricular block (AVB), incomplete and complete right bundle branch block (IRBBB and CRBBB), left anterior hemiblock (LAH), multifocal ventricular extrasystole (MVE), or junctional rhythm (JR) were considered abnormal. The following abnormalities were considered as borderline: atrial extrasystole, junctional extrasystole, unifocal and non repetitive ventricular extrasystole, and R waves in left precordial leads without pattern of ventricular strain in adults >35 years old. The other tracings were considered as normal ECG. IgG antibodies anti-T. cruzi - Specific anti-T. cruzi IgG's were assessed in three assays except for five cases where only two tests were available. Immunofluorescence (IF) was performed at IBBA (Instituto Boliviano de Biología de Altura). Two ELISA assays were performed in two laboratories: IBBA (ELISA-IBBA) and Institut Pasteur Paris (ELISA-IP). The methodologies and the cut values of the three tests were previously described (Wincker et al. 1997, Aznar et al. 1997). ELISA values were expressed as ratio (optical density value of each sample/optical density value of cut value) for statistical analysis. The serological diagnosis of Chagas infection was based on the positivity or negativity of at least two out of three tests. Antibodies against SAPA recombinant protein - Anti-SAPA antibodies were investigated among the total population (except 23 missing cases) using the fusion glutathion S-transferase/shed acute phase antigen (GST/SAPA) previously purified from T. cruzi (Ibañez et al. 1987, Smith & Johnson 1988, Affranchino et al. 1989, Brenière et al. 1997). The current study included 266 sera from children previously tested and 212 additional ones from older patients (Brenière et al. 1997). Briefly, IgG antibodies were detected by ELISA, and SAPA optical density of each sample, was determined by the difference of values obtained by GST-SAPA-ELISA and GST-ELISA as control. The cut-off value for anti-SAPA was 0.38 (Brenière et al. 1997). Antibodies against R-13 peptide - Sera from 469 individuals studied, selected at random, were tested twice for IgG anti-R-13 antibodies by ELISA (Aznar et al. 1995). In each test the samples were assayed in duplicate. The antigen was the synthetic peptide corresponding to the C-terminal sequence (EEEDDDMGFGLFD) of T. cruzi ribosomal P-protein (Aznar et al. 1995). Cut-off values were calculated, in each protocol, as the mean optical density values obtained from 60 control sera + 2 SD. Control sera were represented by 40 T. cruzi negative Bolivian sera and 20 sera from Caucasian individuals from a French blood bank. PCR identification of clonet 20 and 39 - The recognition of clonet 20 and 39 was done by hybridization of the PCR products by clonet specific kDNA probes named 20 and 39 as previously described (Brenière et al. 1998). PCR was applied on 372 blood samples including 209 chagasic patients. Part of the sample was tested previously (Brenière et al. 1998). Statistical tests - Statistics were computed by the Statix package. Prevalence rates of Chagas infection were calculated in different age classes and the correlation between prevalence and middle class age determined by the Pearson correlation test. c2 test was used to compare distributions between several categories and c2 Yates correction was applied when at least one of the expected values was < 5. The non parametric test of Kruskal-Wallis was applied to compare average values obtained for two categories. RESULTS
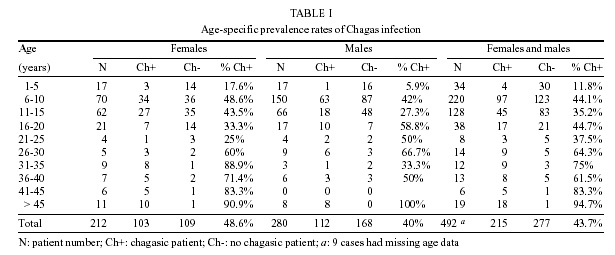
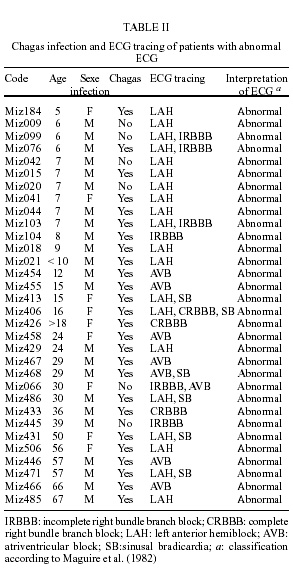
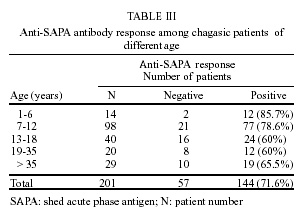
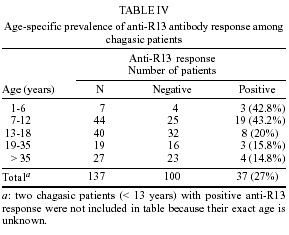
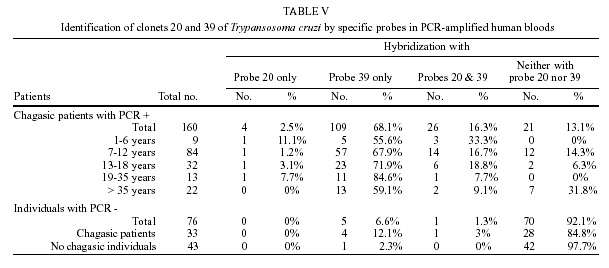
Chagas infection - Two hundred and seventeen individuals out of 501 (43.3%) were positive in at least two of the three serological tests detecting total specific parasite IgG antibodies and were considered as chagasic patients. The accordance of the three tests was 94.7%. Three young children with negative serology were also classified as chagasic: two with evidence of T. cruzi parasitaemia by buffy coat and 1 with positive PCR (Wincker et al. 1997). One adult patient with negative serology was also PCR positive. Finally, a total of 221 patients were classified as chagasic in this study (44.1%). Chagas infection rates increased according to the age of patients from 11.8% to 94.7% (Table I, correlation coefficient = 0.93, p = 10-4) and were not significantly different for male and female (40% and 48.6%, respectively; c2 = 3.29, df = 1, p = 0.07). Cardiac pathology - Table II summarized the characteristics of patients presenting abnormal ECG tracing (32 cases). The other 200 individuals had ECG tracing considered as normal. Among the 232 studied individuals, abnormal ECG was statistically associated with Chagas infection (c2 = 11.8, df = 1, p = 0.0006) and this association was already present among individuals younger than 13 years (c2 = 5.41, df = 1, p = 0.02) (not shown). Moreover, the prevalence of cardiac electric abnormalities was not significantly different among the following age groups: 13 to 18 years old, 19 to 35 years old and >35 years old groups (c2 = 0.38, df = 2, p = 0.83). Only among adult patients (> 25 years old), ECG abnormalities were more common in men than in women (odd ratio = 4.4). No differences of anti-T. cruzi antibodies rates were observed between patients with or without cardiac abnormalities: the Kruskal-Wallis non parametric test was applied to the ELISA-IBBA and ELISA-IP (p = 0.55 and p = 0.20 respectively) and similarly for the IF test (titers £ 1/64 versus titers > 1/64; c2 = 3.3, df = 1, p = 0.07). The most frequent ECG alteration was LAH (61.5% of patients) and the others were present in around 23-27%. More than one alteration was observed among 42% of patients. Finally, 21% of chagasic patients presented an abnormal ECG (26 cases of 123). Anti-SAPA IgG response - The mean ratio of optical density values were 1.8 ± 1.14 and 0.31 ± 0.35 for chagasic and non chagasic individuals respectively. Anti-SAPA antibodies were shown in 72% of chagasic patients and were significantly associated with T. cruzi infection (c2 = 236.4, df = 1, p < 10-4 ). Among chagasic patients, anti-SAPA response was independent of sex (c2 = 3.76, df = 1, p = 0.052) and ECG tracings (c2 = 0.01, df = 1, p = 0.91). Moreover, similar optical density rates were observed for chagasic patients with abnormal and normal ECG (1.84 ± 1.18 and 1.62 ± 1.06 respectively; Kruskal-Wallis test, p = 0.37; not shown). Table III showed that anti-SAPA response was more frequent among chagasic patients < 13 years old than among older (c2 = 7.62, df = 1, p = 0.005), but remained elevated among adult patients. Anti-R-13 IgG response - Twice ELISA assessed anti-R-13 antibodies and the accordance between both assays was of 81.2%. Individuals presenting disagreement were discarded from the analysis and finally, 381 individuals were included. Anti-R-13 antibodies were exclusively detected in chagasic patients (39 patients among 142 tested) demonstrating a strong association between anti-R-13 response and T. cruzi infection (c2 = 73.1, df = 1, p < 10-4). Anti-R-13 antibodies response among chagasic patients, was not related to ECG abnormalities (c2 = 0.98, df = 1, p = 0.32) and sex (c2 = 0.01, df = 1, p = 0.93). Moreover, the anti-R-13 antibodies ratios were not different between the five chagasic patients with abnormal ECG (mean = 2.1 ± 0.9) and the 12 patients with normal ECG (mean = 2.55 ± 1.2), p = 0.53, (Kruskal-Wallis test). Surprisingly, the percentage of chagasic patients with anti-R-13 antibodies was different according to the age (Table IV, c2 Yates = 11.30, df = 4, p < 0.05). It is worth noting that more chagasic patients < 13 years old (41.4%) than older patients > 12 years old (17.4%) presented a positive response (c2 = 10.05, df = 1, p = 0.0015). Furthermore, the antibody ratio was significantly increased among the younger population (< 13 years old, m = 3.3 ± 1.9; > 12 years old, m = 2.3 ± 1.4, p = 0.009, Kruskal-Wallis test). Detection of clonet 20 and 39 in patient bloods - PCR detection of clonet 20 and 39 was applied among 372 individuals including 209 chagasic patients. PCR was positive (presence of 320 bp amplified band) in 83.8% of chagasic patients, and its prevalence was independent of the ECG tracing (c2 = 1, df = 1, p = 0.31) and sex (c2 = 0.29, df = 1, p = 0.59). Higher percentage of positive PCR was observed in young patients < 13 years than in older (c2 = 16.72, df = 1, p < 10-4). Table V summarized the hybridization results of positive PCR products (163 cases), and negatives ones (33 from randomly selected chagasic patients and 43 from non chagasic individuals as control) with probes 20 and 39, after their transfer on nylon membranes. Part of the sample (composed of 137 children < 10 years old) was previously tested, and the additional results confirmed the major prevalence of clonet 39 over clonet 20 in the blood of chagasic patients of any age in this population. Clonet 39 was detected in 77.8% of patients > 18 years old and only 11.1% presented double infections with clonet 20. Six PCR negative samples presented a positive hybridization of the 320 bp band with probe 39 only (five cases) and with both probes (one case); all these patients had a positive serology except one (Table V). Moreover, no significant association of a particular clonet or mixed infection with ECG tracing or sex were observed. The anti-R13 response was analyzed according to the clonets detected in blood patients and significant differences were observed: 37% of the patients infected by clonet 39 (94 cases) had anti-R13 antibodies contrasting with only 6% of the patients (16 cases) without clonet 39 (c2 Yates = 4.64, df = 1, p = 0.031).
ACKNOWLEDGEMENTS
To Fernando Vargas (Instituto Boliviano de Biología de Altura), José Luis Alcazar and Ramiro Fuentes (Cochabamba University) for technical assistance in field and laboratory. To Daniel Sanchez (Fundación Campomar, Buenos Aires) for providing the SAPA recombinant protein, and to Dr Gerardo Antezana (Instituto Boliviano de Biología de Altura, La Paz Bolivia) for revision of the electrocardiographic tracings. REFERENCES
© 2002 Instituto Oswaldo Cruz - Fiocruz
The following images related to this document are available:Photo images[oc02056t2.jpg] [oc02056t5.jpg] [oc02056t1.jpg] [oc02056t4.jpg] [oc02056t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}