 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(3) 2002, pp. 301-305 Hepatitis A Outbreak in a Public School in Rio de Janeiro, Brazil Livia Melo Villar/+, Maria do Carmo Esteves da Costa*, Vanessa Salete de Paula, Ana Maria Coimbra Gaspar
Departamento de Virologia, Instituto
Oswaldo Cruz-Fiocruz , Av. Brasil 4365, 21045-900 Rio de Janeiro , RJ, Brasil
* Núcleo de Estudos de Saúde Coletiva, UFRJ, Rio de
Janeiro, RJ, Brasil This study was supported by CNPq. Received 26 June 2001 Code Number: oc02058
From June 1 to July 1 1999, an outbreak involving 25 cases of hepatitis A occurred in a public school in Rio de Janeiro, Brazil. Since these cases were notified to the State Health Department, the National Reference Center for Hepatitis Viruses (CNRHV) was required to investigate the extent of hepatitis A virus (HAV) dissemination. Blood samples from all students were tested for IgM and total anti-HAV antibodies using a commercial enzyme-linked immunoassay (ELISA). At the same time, a questionnaire was completed in order to identify possible risk factors for HAV infection. The environmental investigation showed that there was no fecal contamination of the water supply. The epidemiological investigation demonstrated that almost 50% of this population was susceptible to HAV infection and probably person-to-person transmission was the principal mode of virus dissemination. In this situation, a massive vaccination campaign could control the HAV infection.
Key words: hepatitis A virus - outbreak - seroepidemiology - public school - Rio de Janeiro - Brazil
Hepatitis A virus (HAV) infection has a worldwide distribution and is transmitted by the fecal-oral route. The prevalence of this infectious disease is closely tied to socioeconomic level, being higher among people of lower socioeconomic status (Hadler 1991). Three epidemiological patterns have been described worldwide. In high endemicity areas with poor sanitary conditions, all children older than 10 years are immune to HAV. In these regions, outbreaks of the disease are uncommon and morbidity is low because in most children the infection is asymptomatic. In developed countries with better sanitary facilities, exposure to HAV during childhood is less common. In these areas, there are large numbers of susceptible adults creating the potential for outbreaks. Finally, developing countries demonstrate an intermediate endemicity with a growing number of adolescents and young adults susceptible to HAV infection. This situation is due to the fact that improvements in sanitary conditions reduced the exposure to HAV in early childhood although the virus has not been eliminated from the environment (Hadler 1991) . Hepatitis A has been a major public health problem in many countries, especially in areas where infection patterns are changing from hyperendemic to hypoendemic (Barzaga 2000, Tanaka 2000, Tufenkeji 2000, Ciancara 2000). Brazil has been an area of high endemicity where infection occurs mainly in children up to 5 years of age (Pannuti et al. 1985, Abuzwaida et al. 1987, Bensabath et al. 1987) . However with the general improvements in hygiene and sanitation standards, the level of HAV infection has declined dramatically in recent years and in some urban regions of Brazil has shifted from a high to an intermediate endemicity status. Hepatitis A was responsible for more than 60% of the acute cases of hepatitis diagnosed at National Reference Center for Hepatitis Viruses (CNRHV) (Gaspar et al. 1996) but 50% of these cases involved persons older than 10 years. Vitral et al. (1998a) demonstrated that the prevalence of anti-HAV among Rio de Janeiro students was 31%, and even in the communities with poor sanitary conditions, almost 50% of the children were non-immune to HAV infection (Vitral 1998b). This new epidemiological pattern has increased the number of susceptible people and has created the potential for large-scale epidemics. On June 1999 the Health Secretary of Rio de Janeiro received reports of 19 clinical cases of hepatitis A. All cases were children who attended a public school in Grajaú, north area of the city of Rio de Janeiro. This study was designed to describe this outbreak and to analyze the possible risk factors for hepatitis A infection in this community. MATERIALS AND METHODS
Study population - This outbreak occurred in a public school situated at Grajaú, north area of the city of Rio de Janeiro. At the moment of this study there were 509 children aged 10-18 years distributed at four classes (5th to 8th grade of elementary education). All of them were tested for total and IgM antibodies anti-HAV. In the school building there were eight rooms, one refectory, three bathrooms (one to males, one to females and the other to teachers). The school works all the day and the children used to eat the meals prepared at the refectory. Formal consent to participate was obtained from parents or guardians of the children. Blood samples were collected on July 1, 1999 and stored at -20°C until tested. Questionnaires - The professionals of CRNHV completed a questionnaire with student information that included age, sex, sanitary conditions of housing (sewage disposal and water supply system), swimming habits (rivers, beaches and waterfalls), number of children and adults in the household, number of rooms in the house, class attendance, recent (within the past month) exposure to persons with hepatitis symptoms, and household income. Laboratory tests - Commercial kits were used according to manufacturer instructions (Organon Teknika, Hepanostika) to detect hepatitis A antibodies (IgM and total anti-HAV). Antibody determination of all serum samples was performed in the laboratory of the Virology Department of Oswaldo Cruz Institute - Fiocruz, Rio de Janeiro, Brazil. Health officers collected water of the public water supply, including the school refectory and toilets, to identify bacterial contamination (total coliforms and fecal coliforms). Statistical analysis - For statistical analysis, frequencies were compared using the c2 test, the Mantel-Haenszel test and the Fisher exact test (one-tailed hypothesis). The strength and precision of the serological status and variables considered were assessed by means of odds ratios (OR) and their 95% confidence intervals (CI). Hypothesis tests were performed using the c2 test, and the chi-test for a linear trend was calculated for ordered categorical variables. To control for potential confounding variables, a multiple logistic regression model was fitted. Statistical analyses were carried out using the Epi INFO 6.01 software (Gahlinger & Abramson 1995). RESULTS
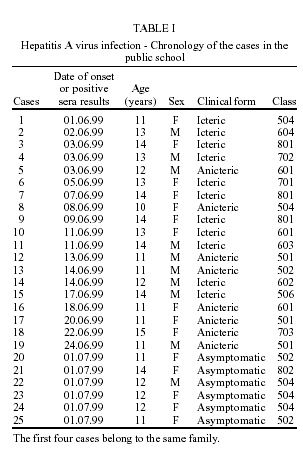
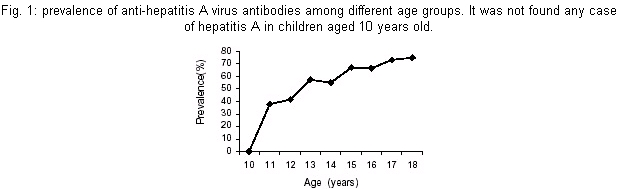
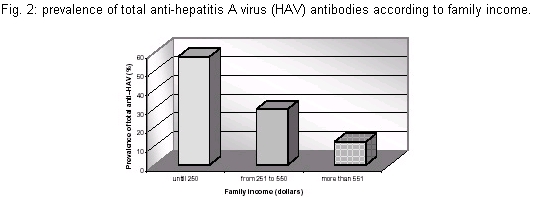
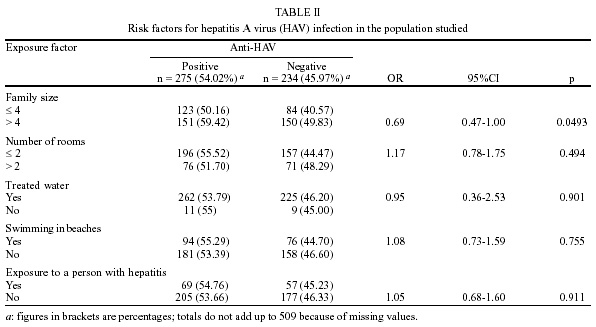
From June 1 to July 1, 1999, 25 cases of hepatitis were identified in the public school in Grajaú, involving 10 males and 15 females. Six of them were asymptomatic, while 11 showed the typical symptoms of acute hepatitis including nausea, vomiting, abdominal pains, diarrhea, fever, hepatomegaly, jaundice, and dark urine; 8 had non-specific anicteric symptoms. There were no deaths. The main features of the cases are reported in Table I. Overall, 54.02% of serum samples were positive for total anti-HAV. The prevalence of anti-HAV increased significantly with age, from 40.8% among children 11 years of age to 75% among children 18 years of age (c2 8GL= 25,40; p = 0.0013) (Fig. 1). No differences in anti-HAV prevalence was observed between males and females (OR = 0.91; 95% CI = 0.69-1.32). HAV exposure was significantly associated with family income (c2 2GL = 18.84; p = 0.00008) as shown in Fig. 2. The prevalence of total anti-HAV antibodies was lower at children with higher family income. Another important variable studied was family size, with anti-HAV prevalence being higher among students living in houses with more than four persons (p = 0.0493). No significant difference was observed when variables such as number of rooms in the home (p = 0.494) and availability of treated water (p = 0.901) were analyzed according to the prevalence of total anti-HAV antibodies (Table II). Other variables analyzed were previous contact with a person with jaundice and going to the beach. However, there was no association between these factors and hepatitis A infection. DISCUSSION
In recent years several outbreaks have occurred in developing countries like Brazil, mainly in schools (Sinlaparatsamee et al. 1995, Leoni et al. 1998, Pebody et al. 1998). Schools constitute an important source of transmission of enteric viruses especially in countries undergoing socioeconomic development. These countries generally experience improvements in public health measures, such as provision of clean water and improved sanitary practices. These improvements lead to a reduction in childhood prevalence of HAV, and as the prevalence diminishes in children, adolescents and young adults become increasingly susceptible to HAV infection. So this new situation creates the potential for outbreaks like the one documented in this school. The description of the outbreak studied can be summarized as follows: the disease appeared in a non-specific form in the index case and was not immediately diagnosed, so this child continued to frequent the school and possibly disseminating the virus in the population studied. The first notification was made on June 11 but, as shown in Table I, the index case had the initial symptoms on June 1, so this child might have gone to school during this interval. The first case attended class 504 and initially the infection was unrecognized. Then this student continued to frequent the school, consequently disseminating HAV infection in his class and later throughout the community. Furthermore it was observed that the first four cases belong to the same family and all of them had the icteric form of the disease but they still continued to frequent the school. These children lived at a house with adequate sewage disposal but with only one room, so the virus could disseminate rapidly in this environment. This fact suggests that person-to-person transmission happened in this family and after to all the community since almost half of this population was still susceptible to HAV infection (46.9%). The latest data from Viral Hepatitis Surveillance Program indicates that contact with a person infected with hepatitis A is the most common identifiable source of infection (22%), on the other hand only 2% of the cases were attributed to ingestion of contaminated food or water (Cuthbert 2001). Moreover the asymptomatic cases were also important because the children continued to go to school, where they could disseminate the virus. The importance of this unrecognized infection was previously demonstrated in other studies (CDC 1987, Staes et al. 2000). Some risk factors were analyzed to identify the possible sources of the infection. Swimming at the beach was an important factor because there are a lot of beaches in Rio de Janeiro and at the time of this outbreak, swimming was forbidden in many of them. However, most of the children did not used to swim at the beach, and therefore this hypothesis was not take into consideration. The association between water supply and the prevalence of anti-HAV were analyzed but it was not significant because the majority of the children reported that their homes had treated water and appropriate sewage. Nevertheless, the water of the school could be contaminated and therefore a local entity responsible for sewage treatment (Cedae) analyzed the school water to determine possible contamination. Since fecal contamination was found to be absent, HAV detection was not investigated. On this basis, we can not state for sure that the school water was not contaminated with the virus. Probably, the poor hygienic conditions observed in school bathrooms and the hygienically incorrect behavior of the pupils, especially the younger ones, led to the spreading of the virus in the school community. The bathrooms were extremely dirty and some children used to eliminate the stools at the floor and probably they did not wash their hands. Rajaratnam et al. (1992) and Leoni et al. (1998) revealed that the school toilets were the source of transmission of HAV infection. In this study we observed a higher prevalence of anti-HAV antibodies in children at lower socioeconomic status, as also reported by Rajan et al. (1998) and Riedemann et al. (1998). Although they have reported to have sewage disposal and water supply system, we can not affirm that these children live in homes with adequate conditions of hygiene. In this situation the virus could spread rapidly and one child with asymptomatic infection could frequent the school and transmit the virus to susceptible persons, as also demonstrated by Smith et al. (1997) and Shapiro et al. (1992). We also found an increasing prevalence of anti-HAV antibodies according with family size. In the family setting, HAV virus is transmitted by the fecal contamination of hands and fomites. Crowding may increase the chance of infectious contacts but also functions as a surrogate for lower socioeconomic status and hygiene standards. In this outbreak this hypothesis was very important since the first four cases happened at the same family. So one child could be acquired the infection at home and could disseminate the virus to the other students. The change in the epidemiology of HAV in Brazil implies the need for new strategies to eradicate HAV infection. In this outbreak, vaccination was administered to all the persons to control the infection, and after this procedure no more cases occurred as it was demonstrated by laboratory tests. Any children had received immunoglobulin previously and only the vaccination was introduced to eradicate the infection. Zamir et al. (2001) demonstrated that postexposure administration of immune globulin may diminish but not entirely arrest the transmission of HAV in community-wide outbreaks. The inactivated vaccine was demonstrated to be highly effective during an outbreak and when given in massive vaccination programs (Werzberger et al. 1992, Innis et al. 1994, McMahon et al. 1996, Bonanni et al. 1998). The vaccination included all susceptible children and school personnel on day July 1 and it consisted of three doses of pediatric HAVRIX (360 Units/dose) (Smith Kline Beecham, Rixensart, Belgium) for children, and of a dose of HAVRIX 1440 for adults. Young children frequently serve as a source of HAV infection for older children and young adults, suggesting that vaccination of young children might also decrease the incidence among older groups. In developing countries, the vaccine should play a vital role, especially during an epidemic. The use of immunoglobulin can not be discarded because this measure is important in some situations. However the administration of vaccine offers a great number of benefits since no more cases were documented after this schedule by any report. In this situation the government has to study the cost-benefit ratio of the hepatitis A vaccine and has to invest in health education and information programs. REFERENCES
© 2002 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc02058t1.jpg] [oc02058t2.jpg] [oc02058f1.jpg] [oc02058f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}