 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(3) 2002, pp. 395-399 Nematode Infections Are Risk Factors for Staphylococcal Infection in Children Sandra F Moreira-Silva, Alba LA Leite, Eliana F Brito, Fausto EL Pereira*/+
Unidade de Doenças Infecciosas,
Hospital Infantil Nossa Senhora da Glória, Vitória, ES, Brasil
*Núcleo de Doenças Infecciosas, CBM, UFES, Av. Marechal Campos
1468, 29040-091 Vitória, ES, Brasil This research was supported by Facitec (Science and Technology Research Agency, Vitória, Espírito Santo, Brazil). Received 28 June 2001 Code Number: oc02075
Nematode infection may be a risk factor for pyogenic liver abscess in children and we hypothesized that the immunomodulation induced by those parasites would be a risk factor for any staphylococcal infection in children. The present study was designed to compare, within the same hospital, the frequency of intestinal nematodes and Toxocara infection in children with and without staphylococcal infections. From October 1997 to February 1998, 80 children with staphylococcal infection and 110 children with other diseases were submitted to fecal examination, serology for Toxocara sp., evaluation of plasma immunoglobulin levels, and eosinophil counts. Mean age, gender distribution, birthplace, and socioeconomic conditions did not differ significantly between the two groups. Frequency of intestinal nematodes and positive serology for Toxocara, were remarkably higher in children with staphylococcal infections than in the non-staphylococcal group. There was a significant correlation between intestinal nematodes or Toxocara infection and staphylococcal infection in children, reinforced by higher eosinophil counts and higher IgE levels in these children than in the control group. One possible explanation for this association would be the enhancement of bacterial infection by the immunomodulation induced by helminth infections, due to strong activation of the Th2 subset of lymphocytes by antigens from larvae and adult worms.
Key words: nematodes - toxocariasis - helminthiasis - staphylococcus In developed countries, immunodeficiency, foreign bodies, and impairment of inborn immune mechanisms are the main predisposing factors for staphylococcal infection (Feigin & Cherry 1992). In developing countries, where staphylococcal infection in children appears to be more frequent in certain diseases, i.e. tropical pyomyositis (Gambhir et al. 1992) and pyogenic liver abscess (Hendricks et al. 1997), malnutrition is considered the main risk factor. Lambertucci et al. (1990) and Teixeira et al. (1996) reported an association of acute toxemic schistosomiasis with pyogenic liver abscess. This finding was reproduced experimentally in mice infected with Schistosoma mansoni and inoculated by intravenous route with Staphylococcus aureus. These authors concluded that immunomodu-lation induced by the infection and trapping of bacteria in granulomas may explain the observed association. In Vitória, State of Espírito Santo, Brazil, we reported that pyogenic liver abscess in children is frequently associated with peripheral eosinophilia, intestinal nematodes (Ferreira et al. 1996), and Toxocara infection (Pereira et al. 1999, Moreira-Silva & Pereira 2000). These observations led us to hypothesize that such helminthic infections are risk factors for liver abscess by the same mechanisms proposed by Lambertucci et al. (1990), and Teixeira et al. (1996), for acute schistosomiasis. Also a relationship of pyomiositis and pyogenic liver abscess with Toxocara infection was reported in Belo Horizonte, State of Minas Gerais, Brazil (Rayes et al. 2000, 2001). Since staphylococcal infections other than pyogenic liver abscess are frequent in children admitted to the "Nossa Senhora da Glória" Children's Hospital, we propose that nematode infection is a predisposing factor for all these infections. To test this hypothesis, we studied the occurrence of intestinal nematodes and Toxocara infection in children with staphylococcal infection as compared to children with other diseases admitted to the "Nossa Senhora da Glória" Children's Hospital. PATIENTS AND METHODS
The "Nossa Senhora da Glória" Children's Hospital is a pediatric reference center belonging to the public health care system. In the last three years, the mean number of admissions has been 2,800 patients/year, and 60% of patients come from the outskirts of Greater Metropolitan Vitória (Vitória, Vila Velha, Cariacica, Serra, and Viana). The study employed a case-control design, which included 80 children with various staphylococcal infections and 110 children with other diseases admitted to different wards in the Children's Hospital from October 1996 to February 1998. The only exclusion criterion was age under one year, due to the lower risk of helminth infection. All the children were from lower-income families, and over 50% were from the urban periphery of Greater Metropolitan Vitória, where they were subjected to the same poor living conditions. The staphylococcal infections diagnosed included pyoarthritis, pyomyositis, liver abscess, skin abscess, otitis, and pneumonitis with or without sepsis. The control group included neoplasms, tuberculosis, meningitis, viral infections, and streptococcal infections. The control group was randomized as follows: twice a week children admitted to various wards the day before, with diseases other than staphylococcal infection, were included as controls. Diagnosis of staphylococcal infection was confirmed by blood or exudate culture. In the control group, all bacterial diseases were confirmed by blood or exudate culture to exclude staphylococcal infection. Three methods were employed for the stool examination: Hoffmann-Pons-Janer, Baermann and Kato-Katz methods (Ash & Oriel 1987). Anti-Toxocara antibodies were investigated with an immunoenzymatic method (ELISA IgG), using a T. canis excretory-secretory antigen obtained from second-stage cultivated larvae (De Savigny et al. 1979). All sera were submitted to prior adsorption with Ascaris suum extract for 1 h at 37°C. In accordance with standard values at the laboratory where the serology was performed, results were considered positive for titers over 500. Serum determination of IgG, IgM, and IgA was performed by turbidimetric assay using commercial kits (TurbiquantÒ, Behring). Quantification of total serum IgE was obtained by microparticle enzyme immunoassay using commercial kits (IMxÒ Total IgE Assay, Abbott Laboratories). Blood counts were performed by routine automatic methods. At least two blood counts were performed: one at admission and the other before discharge. The research protocol was reviewed and approved by the Ethics Committee of the Biomedical Center, Federal University of Espírito Santo. Statistical comparisons were calculated using EpiInfo version 6.1, and differences were considered significant for p values under 0.05. RESULTS
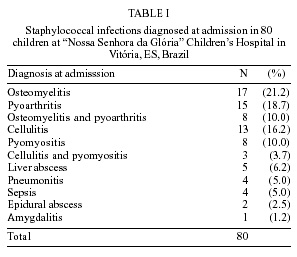
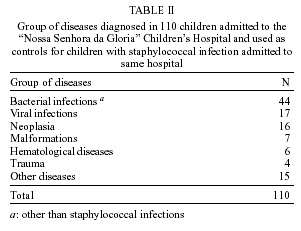
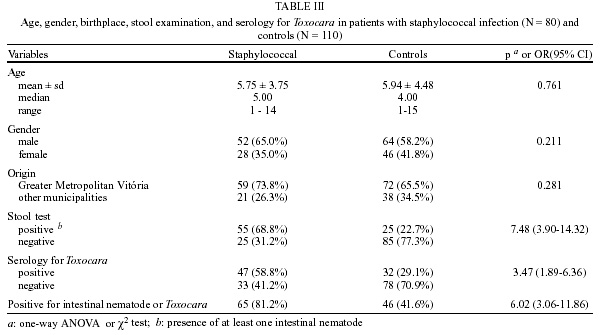
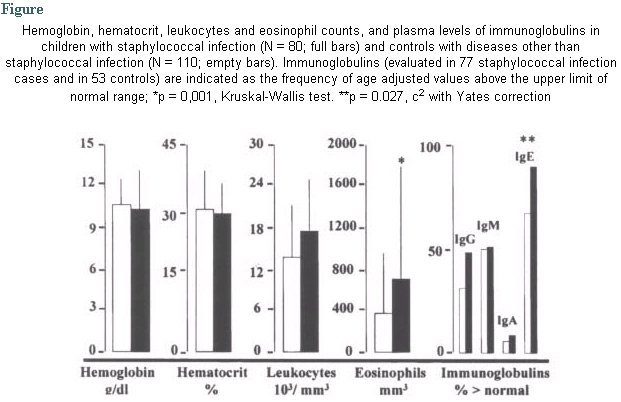
The diseases diagnosed in 80 children with staphylococcal infection are summarized in Table I. The diseases diagnosed in the control group are listed in Table II. Data on age sex, birthplace, frequency of intestinal helminths, and Toxocara serology are shown in Table III. There were significant differences between the two groups in the frequency of intestinal nematodes or positive serology for Toxocara, or both. There was no difference in age, gender distribution, or birthplace between the two groups. Hematocrit, hemoglobin levels, total leukocytes and eosinophil counts, and serum immunoglobulin levels for the two groups are in the Figure. The blood eosinophil counts and the plasma IgE levels were significantly higher in patients with staphylococcal infection. DISCUSSION
There was no significant difference between children with staphylococcal infections and the control group in relation to age, sex or birthplace (Table III). Although we did not investigate all the individual socioeconomic parameters (number of children in each family, mother's working conditions etc.) the two groups belong to the same socioeconomic conditions, since approximately 65% of children in each group came from the urban periphery, where the sanitary conditions are similar (Table I). Nutritional status of the two groups was also similar, as demonstrated by similar values for hemoglobin and hematocrit. Although the two samples showed not significant differences in regard to several variables, we can not rule out several cofounders that are frequent when using in-patients samples. Thus all the conclusions may consider the caveats resulting the assumption that the two samples are comparable. Frequency of intestinal nematodes and Toxocara infection was significantly higher in children with staphylococcal infection. The difference is even greater if we consider nematode infection or Toxocara infection in the two groups: 81.2% in children with staphylococcal infection and 41.6% in the control group (Table III) were infected by an intestinal nematode or showed positive serology for Toxocara. The association of Toxocara infection with intestinal nematodes, especially Ascaris and Toxocara, was frequent, and higher in children with staphylococcal infection than in the control group (72.3% vs. 34.4%, respectively). This association was not due to cross-reaction between Toxocara and Ascaris antigens, because all sera were adsorbed with A. suum antigen before testing. In addition, there were several cases of children with Ascaris infection in which the Toxocara serology was negative in both groups (17 and 12 cases, respectively, in the staphylococcal infection group and in controls). The frequent co-infection with the two nematodes can be explained by the same route of infection (ingestion of eggs) for Toxocara and Ascaris (Lynch et al. 1993). The strong association between helminth infection (intestinal nematodes and/or Toxocara) and staphylococcal infections is reinforced by the higher frequency of peripheral eosinophilia (values above 600 eosinophils/mm3 and higher IgE levels, in children with staphylococcal infection than in the control group). Eosinophilia was significantly higher in children with staphylococcal infection than in the control group at admission, when eosinopenia would be expected because of the stress induced by infection. In fact, the difference in eosinophilia between the two groups increased in the blood count before hospital discharge, when the children's health status was improved (1418 ± 3296 and 518 ± 971 eosinophils/mm3 respectively, in staphylococcal infection cases and controls). Eosinophilia and high IgE levels are typical responses to helminth infection, specially in patients with larval migration through tissues (Allen & Maizels 1996). Although we do not have a definite explanation for this association, we hypothesize that nematode infection enhances staphylococcal infection in children. Considering the data in the literature, we assert that the immunomodulation induced by nematode infection, as manifested by a Th2 shift in the immune response, is the main factor facilitating bacterial infection. Th2 shift in immune response is a hallmark of helminth infection (DelPrete et al. 1991, Bentwich et al. 1996,1999, Allen & Maizels 1996, Finkelman et al. 1997, Kalinkovich et al. 1998) and down-regulation of Th1 responses is demonstrated in some experimental models (Pearlman et al.1993, Ferreira et al. 1995, Allen & Mac Donald 1998, Macedo et al. 1998) and in humans (Kalinkovich et al. 1998, Borkow et al. 2000). The possibility of IgE production in response to Staphylococcus, as in Job's syndrome (Hill & Quie 1974, Scopfer et al. 1980, Donabedian & Gallin 1982, Berger et al. 1988), cannot be ruled out, because helminth infection can act as an adjuvant for IgE production against unrelated antigens (Turner et al. 1979). It is thus possible that in helminth infections, chemotactic defects in leukocytes are induced by high tissue histamine levels, released by mast cells or basophils sensitized with IgE specific for nematode or staphylococcal antigens, as it is admitted in Job's syndrome (Hill & Quie 1974, Berger et al. 1988). A chemotactic defect in neutrophils with improvement after treatment was reported in one child with toxocariasis (Caldwell et al. 1980) . Recently it was demonstrated that chronic immune activation associated with intestinal helminths induced impaired signal transduction and anergy in humans (Borkow et al. 2000). Such impaired immune function may exist in children with nematode infections, reducing the capacity of these children to cope with staphylococcal infections. Another possible explanation for the increased susceptibility to staphylococcal infection in children with nematodes is the trapping of bacteria in granulomas around nematode larvae or antigens. This bacterial trapping would be important for localization of infections, since it occurs in pyogenic liver abscess (Ferreira et al.1996, Pereira et al. 1999, Moreira-Silva & Pereira 2000). As shown in Table I, most staphylococcal infections diagnosed in 80 children had a defined site: pyomyositis, pyoarthritis, osteomyelitis, or pyogenic liver abscess. It is thus possible that granulomas around larvae or antigens occurring in different tissues during Toxocara infection may be areas of bacterial trapping, enhancing the infection. In fact, the spectrum of staphylococcal infection observed here in children with nematode infection is different from that reported in allergic patients in whom the staphylococcal infection is observed in the target organ for allergy, frequently skin and lungs (David et al. 1986). Trapping of bacteria in granulomas and the immunomodulation induced by parasite antigens, acting together, may enhance staphylococcal infection in children with nematode infection, producing higher frequencies of deep abscesses than in atopic patients. Malnutrition was present in children with staphylococcal infection (indicated by hemoglobin levels, Table III), but nutritional status was not different from control patients. While malnutrition may be a predisposing factor for staphylococcal infection in the tropics (Hendricks et al. 1997), the hemoglobin levels were similar, indicating a moderate malnutrition in both groups. It may thus be argued that malnutrition was not a relevant contributing factor for the differences in frequency of staphylococcal infection in these groups. Another possibility that cannot be discarded is the presence of a common genetic defect that predisposes to both nematode and staphylococcal infections. A genetic factor could also predispose patients to nematode infections and allergies, with the two acting together to facilitate staphylococcal infection. Genetic factors enhancing helminthic infections have not been demonstrated in humans (Chan et al. 1994a, b) and the relationship between helminthic infection and allergy is poorly understood: there are conflicting results showing that helminthic infection can increase (Joubert et al. 1980, Bujis et al. 1994, Lynch & DiPrisco 1994) or decrease (Godfrey 1975, Moqbel & Pritchard 1990, Hagel et al, 1993, Lynch et al. 1998) the allergic reactions, depending on the parasite load (Lynch et al. 1998). In this study, we did not investigate the allergic status of the children, neither was a quantitative study of parasite load performed. Further prospective studies are necessary to confirm the association reported here. Also further investigation on chemotactic and microbicidal activity of phagocytes, on production of anti-staphylococcus IgE and on the status of Th1 responses in children with intestinal nematodes or Toxocara infection are necessary to verify the hypothesis described above. REFERENCES
The following images related to this document are available:Photo images[oc02075t1.jpg] [oc02075t2.jpg] [oc02075f1.jpg] [oc02075t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}