 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
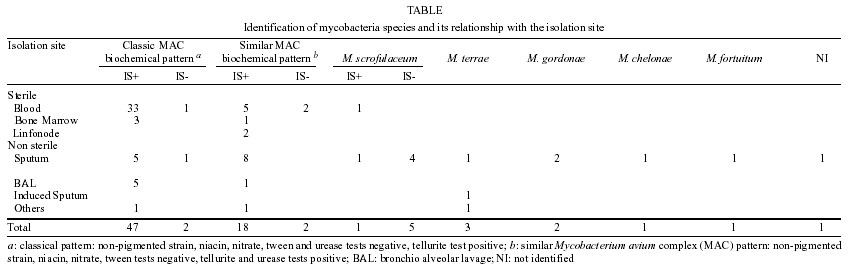
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(5) July 2002, pp. 725-729 Non-tuberculous Mycobacteria I: One Year Clinical Isolates Identification in Tertiary Hospital Aids Reference Center, Rio de Janeiro, Brazil, in Pre Highly Active Antiretroviral Therapy Era Rosa Maria Carvalho Ferreira, Maria Helena Féres Saad*/+, Marlei Gomes da Silva**, Leila de Souza Fonseca** Laboratório de Micobactérias, Hospital Evandro Chagas *Laboratório de Hanseníase, Departamento de Medicina Tropical, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil **Instituto de Microbiologia, CCS, UFRJ, Rio de Janeiro, RJ, Brasil, +Corresponding author. Fax: +55-21-2270.9997. E-mail: saad@ioc.fiocruz.br This publication was supported by grants from CNPq, Papes and Faperj, Brazil, and by a subcontract from the J Hopkins University with funds provided by grant nr 1U19AI45432-01 from NIH. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NIH. Received 28 July 2001 Code Number: oc02138 The aim of this study was to determine the prevalence of non-tuberculous mycobacteria (NTM) isolates at University Hospital, Reference Center for Aids in Rio de Janeiro, Brazil, during one year. We used standard biochemical tests for species identification and IS1245 PCR amplification was applied as a Mycobacterium avium specific identification marker. Four hundred and four specimens from 233 patients yielded acid-fast bacilli growth. M. tuberculosis was identified in 85% of the patients and NTM in 15%. NTM disseminated infection was a common event correlated with human immunodeficiency virus (HIV) infected patients and only in HIV negative patients the source of NTM was non sterile site. M. avium complex (MAC) was biochemically identified in 57.8% (49/83) of NTM isolates, most of them from sterile sites (75.5%), and in 94% (46/49) the IS 1245 marker specific for M. avium was present. Twenty NTM strains showed a MAC biochemical pattern with the exception of a urease-positive (99% of MAC are urease-negative), however IS1245 was detected in 96% of the strains leading to their identification as M. avium. In this group differences in NTM source was not significant. The second most frequently isolated NTM was identified as M. scrofulaceum (7.2%), followed by M. terrae (3.6%), M. gordonae (2.4%), M. chelonae (1.2%), M. fortuitum (1.2%) and one strain which could not be identified. All were IS1245 negative except for one strain identified as M. scrofulaceum. It is interesting to note that non-sterile sites were the major source of these isolates (92.8%). Our finding indicated that M. avium is still the major atypical species among in the MAC isolates recovered from Brazilian Aids patients without highty active antiretroviral therapy schema. Some discrepancies were seen between the identification methods and further investigations must be done to better characterize NTM isolates using other phenotypic and genotypic methods. Key words: non-tuberculous
mycobacteria - tuberculosis - acquired immunodeficiency - IS1245 - biochemical
identification - Non-tuberculous mycobacteria (NTM) or the so-called atypical mycobacteria or mycobacteria other than tuberculosis have been recognized since Koch's time. The recovery of NTM from patients' specimens and from environmental sources is of concern to microbiologists, epidemiologists and physicians. In developed countries, as the incidence of tuberculosis has decreased the occurrence of NTM in pulmonary disease has increased (Ahm et al. 1979, Contreras et al. 1988, Debrunner et al. 1992). Hematogeneous dissemination of NTM has been reported with higher frequency after the advent of the acquired immunodeficiency syndrome (Aids) epidemic. The immunosupressed individual infected by human immunodeficiency virus (HIV) infection became the most significant risk factor for disseminated NTM disease and of these 95% were due to Mycobacterium avium complex (MAC) (Guthertz et al. 1989, Horsburgh 1991). In developing countries little is known about NTM infection, either in Aids or non-Aids patients. In Colombia, which has a low rate of HIV infection, the prevalence of NTM isolates among inpatients has decreased slightly from 5% in 1994 to 4% in 2000, mainly among HIV patients (Murcia-Aranguren et al. 2001). In Brazil, which harbors the highest rate of HIV infection in Latin America (WHO 2000), most available data on NTM isolates was reported in the post Aids period. Usually NTM have not been identified to the species level and the true prevalence of this disease is not clearly known. The recognition of the occurrence of NTM in Aids patients was first reported in the State of São Paulo, with a rate of 18% of MAC in bone marrow of Aids inpatients (Barreto et al. 1993). Fandinho et al. (1997), in a six months survey, in two hospitals in Rio de Janeiro, showed a rate of 37% of MAC in the blood of Aids patients suspected of disseminated mycobacterial infection. Later, Saad et al. (1997), evaluating the distribution of mycobacterial mycosides in clinical isolates from different strain collections, showed that M. avium was the major common opportunistic mycobacterial species isolated from Brazilian Aids patients. In 1999, Conde et al. reported 5.8% of NTM identified from inpatients attended at University Hospital (UFRJ) between 1993-94, of which 60% were HIV positive and 27% of the NTM were identified as belonging to the MAC. The purpose of the present study was to determine the prevalence of NTM isolates at the University Hospital, a Reference Center for Aids in Rio de Janeiro, during the period 1996 to 1997, just before the introduction of highly active antiretroviral therapy (HAART). For strain identification we used classic biochemical tests and for the first time, PCR amplification of IS1245 was used in a prospective study as a species-specific identification marker for M. avium (Guerrero et al. 1995). MATERIALS AND METHODS Setting - The Clementino Fraga Filho University Hospital, is a tertiary-care unit with 500-beds that serves as an Aids reference center in Rio de Janeiro city. It has full in and outpatient specialized units, including a Pneumology Service to attend, among other pulmonary diseases, tuberculosis. Patients - During the period of the study (August 1996 to July 1997) all inpatients or outpatients who attended the hospital with suspected mycobacteriosis had clinical specimens submitted to the Central Bacteriology Laboratory for isolation of mycobacteria. Patient's medical records were recovered for clinical and demographic information. Most of the patients included in this study were not on the HAART schema. HIV status was determined by ELISA test (Organon Teknica, Boxtei, The Netherland) and by western blot (Dupont, Wilmington, USA). Only patients who gave written consent had the HIV test performed. Laboratory procedures - Clinical specimens obtained from sterile body sites, such as cerebral fluid spinal, pleural fluid and ascitic liquid were concentrated by 3,000 x g centrifugation for 20 min and cultured in Löewenstein-Jensen (LJ) medium without previous treatment. Biopsy material (Bp) was smashed in sterilized graal with 1 ml sterile NaCl 0.8% and centrifuged as above. Blood and bone marrow were submitted to a lysis centrifugation method as described by Fandinho et al. (1997). All patients' specimens from non-sterile body sites, including sputum, induced sputum, bronchio alveolar lavage and urine were decontaminated with N-acetyl-L-cysteine-NaOH (Kubica et al. 1963). After decontamination the pellet was submitted to Ziehl-Neelsen staining for microscopy and cultured in conventional LJ medium slant under incubation at 37°C for eight weeks. Mycobacterial identification to species level was done by standard biochemical methods: niacin production, nitrate reduction, catalase activity, tellurite reduction, tween 80 hydrolysis and urease activity (Kent & Kubica 1985). For M. avium differentiation in strains biochemically identified as MAC, IS1245 in house PCR amplification was employed as described by Saad et al. (1999). RESULTS General findings - From August 1996 to July 1997 the central bacteriology laboratory of the University Hospital in Rio de Janeiro received 3,641 clinical samples for mycobacterial culture of which 506 specimens from 260 patients yielded ABF growth. This reflects 13.9% culture positivity and a positive specimen average of 1.9 per patient. Forty-two strains from 27 patients were excluded by contaminatio and/or were non viable. The initial screening of ABF growth by colony morphology and by biochemical tests such as niacin production, nitrate reduction and catalase activity, made it possible to separate a large group of patients harboring M. tuberculosis (198/233; 85%) and a group that yielded mycobacteria other than tuberculosis (35/233; 15%). One patient had simultaneously infection with M. tuberculosis and NTM. M. tuberculosis, as expected, was most often isolated from pulmonary specimens (78.8%) followed by blodd and bone marrow aspirate (7.8%) and fro mpleural specimens (7.3%). HOwever, NTM strains were most frequently isolated from sterile sites such as blood, bone marrow asporate and lumph node specimens (57.8%), while only 38.5% of NTM isolates were identified in pulmonary specimens. NTM findings -- The 83 mycobacterial positive cultures classified as NTM were submitted to a complementary speciation by conventional biochemical test (tellurite reduction, tween 80 hydrolyze and urease activity). As depicted in the Table, 49 out of 83 (57.8%) NTM strains showed the classic MAC biochemical pattern. An interesting observation is that the organisms of this group were predominantly isolated from sterile sites including blood and bone marrow aspirate (37/49; 75.5%; p<0.0001). The remaining M. avium was found in non-sterile sites (12/49; 24.5%). Ninety six percent of the MAC strains (47/49) had the 427 base pair fragment PCR amplified from IS1245, a specific marker for M. avium. Three samples could not be amplified by PCR, two were isolated from blood and the other from sputnum. Twenty NTM strains (20/83, 24.1%) showed MAC biochemical pattern concordance with an exception of positive urease activity. However, 90% (18/20) of the strains had positive IS1245 PCR amplification, and M. avium was the final identification despite the urease phenotypic discrepancy. In this group, the proportion of isolates from sterile and non-sterile site was the same 10 from sterile sites and 10 from non-sterile sites. the last 14 NTM isolates were identified as M. scrofulaceum (6/83; 7.2%), M. terrae (3/83;3.6%), M. gordonae (2/83; 2.4%), M. chelonae (1/83; 1.2%), M. fortuitum (1/83; 1.2%) and one strain, which could not be identified. All were negative for IS1245 PCR amplification except one strain identified as M. scrofulaceum. It is interesting to note that non-sterile site were the major source of these strains (13/14; 92.8%). The 83 NTM isolates were obtained from 35 patients, giving an average of 2.37 isolates per patient. The mean age of these patients was 34 years old and male sex pattern accounts for most isolates (23/35; 65.7%). MAC isolates occurred in 21 out of 35 (60%) patients. HIV co-infection was present in 95% (20/21) of these patients, and disseminated infection was a common clinical episode, occurring in 14 patients. In the only HIV negative patient the source of MAC was a non-sterile site. Six of 35 (22.8%) patients harboring M. scrofulaceum, the second most frequently identified species, three patients were HIV positive and only one had disseminated infection. The remaining patients harbored M. terrae (3/35; 8.6%), M.gordonae (2/45; 5.7%), M. chelonae (1/35; 2.8%), M. fortuitum (1/35; 2.8%), and in one patient the mycobacterial strain was not identified. None of them had disseminated infection and two were HIV co-infected. Most of HIV patients were under antiretroviral treatment and only nine patients had been receiving HAART for at least one month. Ten patients had multiple isolates from the different sites or at different sampling periods, which could vary from one day to four months (for the same patient). The multiple isolates were identified as M. avium by phenotypic and genotypic mehtods. Three patients showed at least one M. avium isolate with discrepant PCR IS1245 results from others isolates. The first one had 12 isolates and all but one showed a positive PCR result. The second harbored seven isolates and the PCR negative strain was isolated from blodd and the others from non-sterile site. The last patient had three isolates and, as the second patient, the PCR negative strain was isolated from blood and the two other strains were PCR positive and isolated from non-sterile site. DISCUSSION From August 1996 to July 1997, 260 patients with positive mycobacterial culture yielded 17.8% of NTM isolates. This number is smaller than the rate reported in the United States (20 to 35%) (Horsburgh 1997). The most plausible explanation is the high incidence of tuberculosis in Brazil, which cause a relative low prevalence of non-tuberculosis mycobacterial disease. In fact, it is difficult to compare our data for disease due to NTM with those published in other countries because of variation in the study periods, selection criteria and populations studied (Edwards 1970, O'Brien et al. 1987, Tsukamura et al. 1988, Reich & Johnson 1991, Debrunner et al. 1992, Hosker et al. 1995). Among the few studies done in Brazil, in two mycobacterial isolation was performed only from sterile sites. On the other hand, in the same hospital used in our study, Conde et al. (1999) reported lower occurrence of NTM (5.8% x 15% in the present study), however their analyses focused mainly on respiratory specimens. In contrast to the M. tuberculosis findings, most of our NTM isolates were obtained from sterile sites (57.8%), which confirm the dissemination characteristic of NTM infection in Aids patient, since 72.4% of them were HIV co-infected. This feature is also corroborated by the observation that 61% of NTM isolated were obtained from inpatients or those attended at the emergency room, that represent patients with serious clinical conditions, while only 30% with M. tuberculosis were inpatients. Organisms belonged to M. avium complex comprise two distinct species, M. avium and M. intracellulare. The M. avium complex was the main NTM isolated (83%) and M. avium, identified by PCR amplification of IS1245, was the species most frequently isolated (77.1%). The other studies done in Brazil did identify MAC to the species level and this is the first prospective study on NTM to use a specific M. avium identification marker. Four strains, identified by biochemical test as MAC, showed negative IS1245 PCR amplification. Recently, Oliveira et al. (2000) reported the absence of the IS1245 in a strain from a patient with polyclonal M. avium infection. In the present study IS1245 positive and negative strains were isolated simultaneously from three patients. This finding may represent a relevant aspect related to a polyclonal infection with genetically different stains. The occurrence of polyphenotypic and genotypic in multiples isolates of the same patient has been described previously in Brazilian Aids patients (Saad et al. 1997, 2000), also the description of phenotypic and genotypic variability was recently reported using single colonies from M. avium obtained from Aids patients (Oliveira et al. 2000). Other possible explanations for this finding could be the presence of M. intracellulare, even in those specimens from sterile site or simply technical limitations of the PCR. Although 99% of MAC strains are negative in the urease test, 20 strains in our study showed a positive result; those strains were considered MAC since all but two were IS1245 PCR positive. To clear this question phenotypic and genotypic identification by others methods as HPLC and PRA and molecular fingerprint should be done with those strains. The second most frequently isolated NTM from the studied specimens was M. scrofulaceum. This finding was quite surprising, since in a previous study using mycoside serotype as marker to identify M. avium-intracellulare-scrofulaceum complex in Brazilian isolates from Aids patients, M. avium and M. intracellulare were the most common serotypes obtained (Saad et al. 1997). In this present study, the phenotypic pattern used to differentiate M. scrofulaceum from MAC was pigment production, urease positivity and a negative IS1245 PCR. However, we found some MAC strains with one of the following characteristics positive urease, negative PCR and pigment production. Moreover, pigmented MAC is frequently isolated from Aids patients (Kiehn et al. 1985). Since biochemical tests are not the most powerful and easy typing method for NTM isolates and we used only a few tests; the M. scrofulaceum identification could be due to misinterpretation of the results. The finding of M. scrofulaceum biochemical identification with IS1245 positive may support this suggestion, however to clarify this other phenotypic and genotypic methods must be applied, such as HPLC and PRA. The data shown in this study may provide an indication that NTM infection in Aids patients remains a Pandora's box and further investigation must be done to better characterize NTM isolates using different phenotypic and genotypic methods. Our paper also emphasizes that despite M. tuberculosis is being by far the most important cause of mycobacterial disease, NTM infections must be taken into consideration when dealing with Aids patients without HAART schema. Among the mycobacterial species M. avium seems to be predominantly isolated from hospitalized patients. Investigation in this field is still important and new surveys must be done to evaluate mycobacterial infection positive modulation in patients on HAART (Kirk et al. 2000). Recent results obtained at the Evandro Chagas Hospital-Fiocruz, Rio de Janeiro, showed that MAC and M. tuberculosis infection in Aids patients decrease in those on HAART (pers. commun.). REFERENCES
Copyright 2002 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc02138t1.jpg] |
| |||||||||

{kind=link}