 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
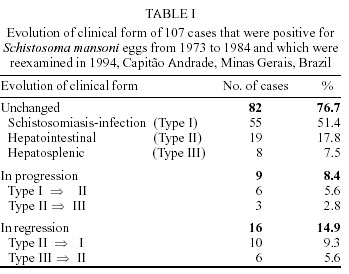
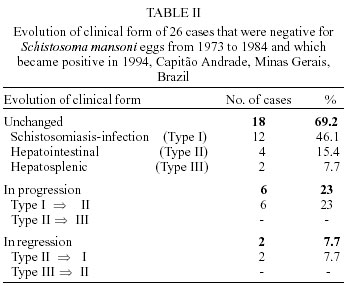
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(5) July 2002, pp. 755-757 SHORT COMMUNICATION Influence of Specific Treatment on the Morbidity of Schistosomiasis Mansoni in an Endemic Area of Minas Gerais, Brazil Maria José Conceição/*/+, J Borges-Pereira* Serviço de Doenças Infecciosas e Parasitárias, Hospital Universitário Clementino Fraga Filho, UFRJ, Rio de Janeiro, RJ, Brasil *Departamento de Medicina Tropical, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil, +Corresponding author. Fax +55-21-2280.3740. Email: conceicao@ioc.fiocruz.br This work was partially supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico - CNPq. Received 2 October 2001 Code Number: oc02144 The authors describe the evolution of schistosomiasis mansoni in inhabitants of Capitão Andrade, Minas Gerais, Brazil, from 1973 to 1994. The prevalence of infection was 60.8% in 1973, 36.2% in 1984, and 27.3% in 1994. The evolution of the clinical forms of the disease in this group was as follows: unchanged in 76.7%, clinical progression in 8.4% and clinical regression in 14.9%. The reduction of the prevalence and severity of Schistosoma mansoni infection over the 21 years period, can be attributed to treatment of infected subjects performed in the area and to the installation of piped water in their dwellings. Key words: schistosomiasis mansoni - clinical evolution - morbidity - treatment - Minas Gerais - Brazil The elevated prevalence and severity of Schistosoma mansoni infection in the area of Itanhomi, Minas Gerais, was first observed in 1972 in the Santa Luzia do Carneiro village, in a pilot sectional survey (Conceição et al. 1976). In 1973 a hyper endemic area was detected in Capitão Andrade, Vale do Rio Doce, Minas Gerais (Figure), with the splenomegaly index of 5.6%. The severity of the clinical forms in the present municipality of Capitão Andrade (Conceição 1976) motivated a longitudinal study that was conducted despite the limitations of case follow-up due to the marked migratory flow of inhabitants into and out of the area. A survey, starting in 1973, was conducted on a group of 1,234 subjects with further re-examinations of 324 inhabitants in 1984 and of 224 in 1994. The study area is located in the municipality of Capitão Andrade. Three stools tests were performed in the patients to verify positivity for S. mansoni eggs according to Kato method modified by Katz et al. (1972). All the subjects were inhabitants of Capitão Andrade. The same two physicians, responsible for the study, examined the individual subjects in all phases of the study without any random selection. The same group of subjects who had been examinated in 1973 and who had not left the study area were re-examined in the subsequent phases of the study. To evaluate the size of liver and the spleen the subjects were examined under the position of Schuster, as well as in the dorsal position (during deep expiration). It was not possible to conduct abdominal ultrasound examinations of subjects in the initial phase of the study (1973), because this technique was not in use on the occasion. Another reason was the absence of electricity in the study area. The patients were included in three groups and it was continued in the subsequent phases of the study: type I - schistosomiasis-infection, with or without intestinal symptoms, which, if present, were moderate and not necessarily attributed to the disease; type II - hepatointestinal form, frequent intestinal symptoms, dysenteric diarrhea and hepatomegaly; and type III - hepatosplenic form, very frequent intestinal symptoms, dysentery and hepatosplenomegaly with or without hematemesis or melena. During the clinical examination information was obtained from the subjects about episodes of fever, epistaxis, digestive bleeding, icterus and alcoholism. The specific therapy was performed in 1984 with oxamniquine, single oral dosis, 15 mg/kg for adults and 20 mg/kg for children. After 60 and 90 days of therapy the fecal examinations were performed for the control of cure. Analysis of variance with emphasis on the analysis of regression were employed to evaluate the progress or regression of hepato and or splenomegaly during the various phases of the study considering age, height and weight of the subjects. The p-value was significant at the 0.05 level. In 1973, the positivity for S. mansoni eggs among the 1,234 inhabitants was 60.8%. Coura et al. (1984) examined 324 subjects from this same groups and obtained a prevalence of 36.2%. In 1994, a review of 224 cases showed a 27.3% prevalence of infected individuals. Of the 224 inhabitants reviewed, 107 were infected in 1984 and 117 were negative. Twenty-eight of the 107 positive subjects (29.1%) continued to be positive for S. mansoni eggs in 1994. Eighty-two of the 107 subjects (76.7%) had an unchanged clinical form. Nine (8.4%) showed progression of the disease as follows: 6 (5.6%) progressed type I (schistosomiasis-infection) to type II (hepatointestinal form) and 3 (2.8%) from type II to type III (hepatosplenic form). Clinical regression occurred in 16 patients (14.9%), 10 of whom (9.3%) regressed from the hepatointestinal to the schistosomiasis-infection form and 6 (5.6%) from the hepatosplenic to the hepatointestinal form (Table I). Nine of the 16 patients with clinical regression (56.2%) reported treatment with oxamniquine. From a total of 117 individual who were negative in 1973 and 1984, 91 were reexamined in 1994 and 26 of them had become positive. Eighteen of these 26 patients (69.2%) maintained the same clinical examination as in the previous stage, with no progression or regression. Six cases (23%) showed progression from the schistosomiasis infection to the hepatointestinal form. Improvement of clinical form occurred in 2 cases (7.6%); both went from the hepatointestinal to the schistosomiasis infection form (Table II). Prata and Bina (1968), in Catinga do Moura, Bahia, during a follow up of 5 years verified a progression of 20 patients over 20 years old from types I and II to type III. To explain the maintenance of the severe forms in Capitão Andrade, the hypothesis of development of splenomegaly in previously infected cases was raised in 1994, a new survey in the area continued to reveal a fall in prevalence from 36.2% in 1984 to 27.3%, as well as dynamic variation in the clinical forms, both with the occurrence of hepato and splenomegaly and with the regression of splenomegaly in 5.6% of cases. Ultrasonography has become an invaluable extension of the clinical investigation of subjects with schistosomiasis, providing direct evidence of the pathological changes in association with this infection (Pinto-Silva & Lambertucci 1986, Pinto-Silva et al. 1994, TDR News 2000). However, the role of the abdominal ultrasonography in the diagnosis of hepatosplenic schistosomiasis was only emphasized after the first stage of this work started in 1973. So, the authors decided to keep the same clinical classification during the three stages of this research. Ultrasound performed in the subsequent phases of the study confirmed the physical examination, but were observed discordance in a total of three cases. How the reinfection would influence the development of splenomegaly in this area? Bina (1995) during a 15 years follow-up in Taquarendi, Bahia, suggested that successive reinfections and specific therapy may have had some influence in the development of the hepatosplenic form of schistosomiasis. Bina (2001) confirmed those results in a paper as a part of the Project on Schistosomiasis in Chapada Diamantina, Bahia, Brazil. However, the main factors related to the maintenance of severe forms in Capitão Andrade are not completely known. It is probable that the reduction in prevalence during this phase of the survey was related to the treatment with oxamniquine, provided by local health organs, in combination with the partial installation of piped water in the dwellings. ACKNOWLEDGMENTS This paper is dedicated to the memory of Mozar José Coelho, who gave the authors his friendship, support and encouragement of research in Capitão Andrade. To Dr JR Coura, for the total assistance and incentive during our career. To Acyr Corrêa, Maria de Lourdes Gomes de Carvalho, Tatiana Fazecas, Debora C Moura, Alvaro P Filho and Andrea Teixeira for their technical assistance throughout the course of this study. To Nelson Chagas from Uerj, for the Statistical Analysis, to Dr John Morey Maurice and José Roque Conceição from Gonzaga University School of Law, Spokane, USA, for the revision of the manuscript. REFERENCES
Copyright 2002 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc02144f1.jpg] [oc02144t1.jpg] [oc02144t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}