 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(6) September 2002, pp. 775-778 Hepatitis C and Hepatitis B Virus Infection in Different Hemodialysis Units in Belo Horizonte, Minas Gerais, Brazil Solange U Busek/*, Élio H Babá*, Hélcio A Tavares Filho**, Lermíno Pimenta***, Abraão Salomão****, Rodrigo Corrêa-Oliveira, Guilherme C Oliveira/*****/+
Centro de Pesquisas René Rachou-Fiocruz,
Av. Augusto de Lima 1715, 30190-002 Belo Horizonte, MG, Brasil *DECBI/NUPEB,
Universidade Federal de Ouro Preto, Ouro Preto, MG, Brasil **Hospital Biocor,
Belo Horizonte, MG, Brasil ***Santa Casa de Misericórdia, Belo Horizonte,
MG, Brasil ****Instituto Mineiro de Nefrologia, Belo Horizonte, MG, Brasil *****Programa
de Pós-Graduação e Pesquisa, Santa Casa de Misericórdia,
Belo Horizonte, MG, Brasil This study was supported by Capes, Ufop and Papes-Fiocruz. Received 26 December 2001 Code Number: oc02148
The prevalence, virological and epidemilogical aspects of the hepatitis C virus (HCV) and the hepatitis B virus (HBV) infections vary among hemodialysis patients in different countries. Aiming at analyzing these aspects of HCV and HBV infections in hemodialysis patients in Belo Horizonte, MG, Brazil, we studied three hemodialysis units including 434 patients. Serology was used to detect anti-HCV and HBsAg. Reverse trancriptase nested polymerase chain reaction (RT-nested-PCR) of the 5'-noncoding region was used to detect circulating HCV RNA and restriction fragment length polymorphism analysis for genotyping. Seroprevalence varied from 26.5% to 11.1% for hepatitis C and from 5.9% to 0% for hepatitis B. Risk factors observed for HBV and/or HCV infections were the number of patients per dialysis unit, duration of treatment, number of clinics attended, number of blood units transfused, and lower level scholarity. Alanine aminotransferase levels were altered with a higher frequency in HBV or HCV seropositive patients. Half of ten patients, negative for anti-HCV, had detectable viremia by RT-nested-PCR, indicating that this technique should be used to confirm infections in this group of patients. The HCV genotype 1 was the most frequently observed, followed by the genotype 2, but no correlation was detected between genotype and clinical or epidemiological data.
Key words: alanine aminotransferase - hepatitis C virus genotype - hemodialysis - hepatitis B - hepatitis C - prevalence - Belo Horizonte - Brazil The hepatitis C and B viruses (HCV and HBV) are highly prevalent in hemodialysis patients (Tokars et al. 1995, Wreghitt 1999). The high levels of prevalence have been related to the duration of the dialysis treatment and the number of blood units transfused (Wreghitt 1999). Nosocomial transmission of HCV and HBV also appears to be an important contributing factor to the spread of these viruses (Castro-Figueiredo et al. 1986, Teles et al. 1998, Wreghitt 1999, Carneiro et al. 2001). The prevalence of the HBV has drastically reduced with control practices, but outbreaks are still frequent and routine screening necessary (Wreghitt 1999, Lewis-Ximenez et al. 2001). The HCV is a positive-stranded RNA molecule of approximately 10,000 nucleotides (Choo et al. 1989). Based on genome sequence, at least six main genotypes, with varying geographical distribution, have been observed for HCV (Takada et al. 1993, McOmish et al. 1994, Bukh et al. 1995). These genotypes appear to be clinically relevant in relation to virulence and chemotherapy response (Hopf et al. 1996). In Brazil, high anti-HCV prevalences within hemodialysis units have been observed (Oliveira GC et al. 1999, Carneiro et al. 2001). The distribution of HCV genotype is similar to that observed in Europe, with the predominance of the genotype 1 followed by the genotype 3 (Oliveira GC et al. 1999, Oliveira MLA et al. 1999). HBV prevalence was found to be highly variable, from 2 to 78% in hemodialysis clinics (Teles et al. 1998). The aim of the present study was to investigate the epidemiological and clinical features of HCV and HBV infections and the distribution of HCV genotypes in hemodialysis patients, in three different hemodialysis units in Belo Horizonte, MG, Brazil. MATERIALS AND METHODS
Patients - Clinical and epidemiological data were obtained from March to December 2000 in three hemodialysis units in Belo Horizonte, MG, Brazil, from a total of 434 hemodialysis patients. Age varied from 18 to 94 with an average of 50 years of age. Male patients comprised 56.3% of the studied population. Patients were under treatment at three different hemodialysis centers, each with 54, 169 and 211 patients. Formal consent to participate was obtained from all patients. The ethical and methodological aspects of this study received Research Ethics Committee approval. Serological assays - Serum samples were tested for anti-HCV by using third-generation enzyme immunoassay (EIA.3.0, Abbott Laboratories, Chicago, IL) (units 1 and 2) or ImmunoComb II (Orgenics, Israel) (unit 3). Samples were tested for HBsAg by ELISA (Auszyme Monoclonal, Abbott Park, IL, USA). Serum alanine aminotransferase (ALT) activity was monthly determined since seroconversion to HCV or HBV by using the ALT-Randox (Randox Laboratories, San Diego, CA). ALT levels were considered to be elevated when 1.5 times above the maximum normal value, 8-40 UI/l. ALT levels were considered intermittent, when observed to be elevated in a single determination, or persistent when elevated for at least three consecutive determinations. Detection and genotyping of HCV RNA - HCV RNA detection was performed by reverse transcriptase nested polymerase chain reaction (RT-nested-PCR) of the 5' non-coding region, and genotyping by restriction fragment length polymorphism (RFLP) of the amplified product, as previously described (Oliveira GC et al. 1999), for all anti-HCV positive patients. For control reactions, in addition to amplifications with no template, we tested 10 random samples of anti-HCV-hemodialysis negative patients. Statistical analysis - Fisher's exact and the Chi-square tests were applied with Yate's correction for the analysis of the data; a < 0.05. RESULTS
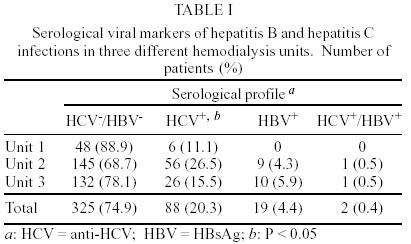
The average prevalence of seropositivity to HCV infection (anti-HCV+), among 434 hemodialysis patients, was 20.3%, 4.6 times higher than that observed for HBV (4.4%). Co-infection was observed in only two patients (0.4%). HCV infection prevalence was significantly different among units (P < 0.05). Unit 2 showed the highest prevalence (26.5%) followed by unit 3 (15.5%) and unit 1 (11.1%). The prevalence of HBV infection (HBsAg+) was similar between units 2 and 3 (4.3 and 5.9% respectively), and unit 1 did not have any case of HBsAg+ (Table I). The prevalence of HCV RNA among 88
HCV seropositive patients was 94.3%. Two out of 10 patients with indeterminate
serology had detec HCV RNA. In addition, of 10 patients with negative serology
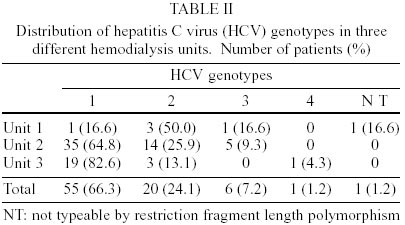
5 had detec HCV RNA. Hepatitis C virus genotype was determined for 83 HCV RNA
positive patients. Genotype 1 was the most common (66.3%), followed by genotype
2 (24.1%) and genotype 3 (7.2%). Genotype 4 was detected in only one patient
(1.2%) and in another patient the amplified fragment was not typeable by RFLP.
Despite the predominance of the genotype 2 in unit 1, there was not a statistically
significant difference in the genotype distribution among the three hemodialysis
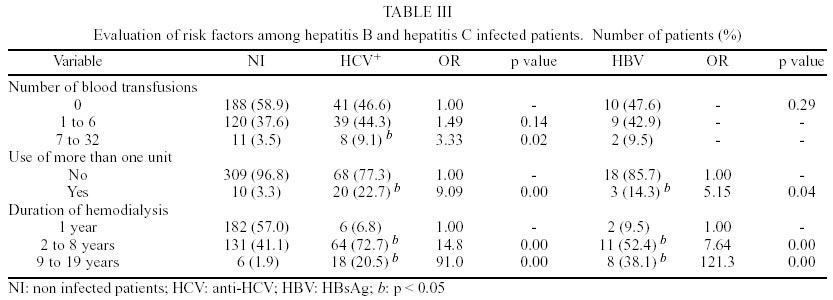
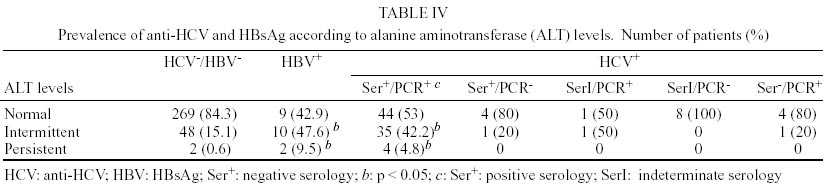
units A higher prevalence of HCV was observed in patients with the lowest educational levels (P < 0.05). No correlation among HCV prevalence and sex, race, place of residence and marital status was observed (data not shown). The use of multiple hemodialysis units and the duration of treatment were important factors for the acquisition of both HCV and HBV infections in dialysis patients. However, an elevated number of blood transfusions (seven or more) were correlated only to the HCV positivity (Table III). A significantly higher number of patients with intermittently or persistently elevated ALT levels were observed for HBsAg+ or anti-HCV viremic and seropositive patients, in comparison with seronegative (HBV and HCV) and/or RT-PCR negative patients (Table IV). No correlation was found between the different genotypes and demographic characteristics, risk factors, ALT, serology, and viremia. DISCUSSION Hemodialysis patients are an important risk group for HCV infection. We observed a lower prevalence of anti-HCV positive (20.3%) patients when compared with other dialysis centers in Brazil (50%) (Oliveira MLA et al. 1999, Carneiro et al. 2001), United States (average = 10.4%) (Tokars et al. 1998), Portugal (48%) (Carrera et al. 1994) and Saudi Arabia (45.5%) (al Nasser et al. 1992). Different prevalences of HCV infection were observed in the three hemodialysis units under study. It is known that different methods of control, cleaning and disinfection of the hemodialysis membranes, machines, instruments and environmental surfaces may interfere with determined prevalences (Wreghitt 1999). We observed that the prevalence was also positively correlated with an increased number of patients under treatment per unit. Another important observation of this study was that patients attending more than one treatment unit had nine times greater risk of being infected by HCV. Higher age and longer duration of hemodialysis treatment were also an important risk factor for HCV infection (Teles et al. 1998, Carneiro et al. 2001). As observed by others, the higher risk for HCV, infection in patients with seven or more blood transfusions, is probably related to poor infection screening and control methods (Wreghitt 1999). Serological tests are used worldwide for the screening of HCV infection. Some of the serological tests have shown up to 10% disagreement with PCR based tests (Garinis et al. 1999). In this paper, we describe confirmation of active infection by RT-nested-PCR in 94.3% of the patients studied. The unconfirmed cases may have been the result of a decrease in viral load observed in this group of patients (Furusyo et al. 2000). The occurrence of HCV RNA detectable in patients with negative anti-HCV can be a consequence of immunossupression with decreased production of antibodies, or the window period of a recent infection (Sharara et al. 1996, Lok & Gunaratnam 1997). Another possibility is the absence, in the serology kits used, of an antigenic variant that is present in the geographic area studied (Dow et al. 1996). Other studies also detected HCV or HBV nucleic acids in anti-HCV negative or HBsAg-negative/IgM anti-HBc-positive hemodialysis patients, respectively (Carneiro et al. 2001, Lewis-Ximenez et al. 2001). The potential problem of a high prevalence of HCV RNA positive patients in an HCV seronegative group deserves to be studied in depth, due to the possible consequences to HCV transmission in hemodialysis centers. The genotype distribution of the HCV isolates in the units studied was not different from those previously reported from the same geographical area (Oliveira GC et al. 1999, Oliveira MLA et al. 1999), with a predominance of the genotype 1. Nonetheless, somewhat elevated prevalence of the HCV genotype 2, which has been shown to be rare in Brazil, especially in unit 1, may suggest nosocomial transmission. One of the important parameters measured in hepatitis virus infected patients are the levels of circulating ALT enzyme. We observed that a higher number of HBsAg+ or HCV positive (RNA and serology) patients had intermittently or persistently elevated ALT levels. However, a large number of these patients had normal ALT levels, indicating that this marker should be used in combination with other variables in the construction of a useful algorithm to determine patient clinical status for HCV and HBV infections.
ACKNOWLEDGEMENTS
To Drs Michele Hostalácio Duarte, Cláudia Ribeiro, André Duarte, Valério Rodrigues, Alcimar Gonçalves dos Santos, Acássia Lippi, Maria Paulina Pinto and the nurses of the three hemodialysis units for their help with collecting patient's information and samples. REFERENCES
Copyright 2002 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc02148t4.jpg] [oc02148t3.jpg] [oc02148t1.jpg] [oc02148t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}