 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(6) September 2002, pp. 783-787 Hantavirus Pulmonary Syndrome in Uberaba, Minas Gerais, Brazil Mario León Silva-Vergara+, José Carlos Costa Júnior, Cristina Hueb Barata, Vítor Guilherme Maluf Curi, Carlos Giovanni Tiveron Júnior, Alan César Teixeira
Disciplina de Doenças Infecciosas
e Parasitárias, Departamento de Clínica Médica, Faculdade
de Medicina do Triângulo Mineiro, Av. Getúlio Guaritá s/nº,
38001-970 Uberaba, MG, Brasil Received 28 December 2001 Code Number: oc02150
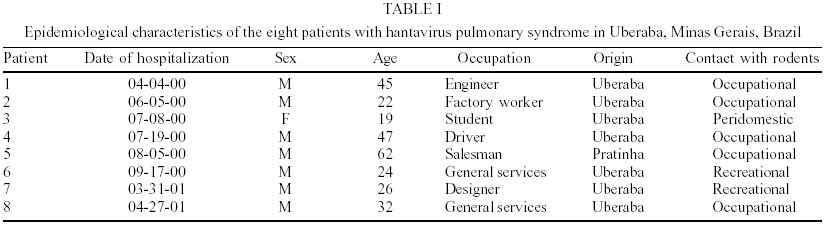
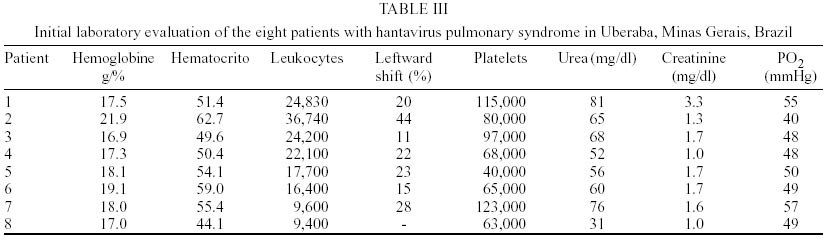
This report describes the epidemiological and clinical-evolutive characteristics of eight patients with hantavirus pulmonary syndrome (HPS) in Uberaba, Minas Gerais, Brazil. A positive history of contact with rodents was present in 100% of the cases. The time between the onset of symptoms and hospital care was, on average, 3.6 days. All patients showed clinical and laboratory findings suggestive of HPS. Elevated urea and creatinine levels were observed in 6 (75%) cases, PO2 was < 60 mmHg in 100% of the cases, and a chest X-ray demonstrated a bilateral interstitial-alveolar infiltrate. The diagnosis was confirmed by the detection of IgM antibodies against Sin Nombre virus by ELISA. Three patients died as a direct consequence of HPS.
Key words: hantavirus - hantavirus pulmonary syndrome/HPS - Sin Nombre virus - Minas Gerais - Brazil Since the report of the first outbreak of hantavirus pulmonary syndrome (HPS) in New Mexico, USA (CDC 1993), more than 200 cases have been notified in that country (Van Bevern 2000). Later on, other countries on the American continent also reported the occurrence of cases, mainly Brazil, Canada, Argentina, Chile, and Paraguay, among others (Lopez et al. 1996, Johnson et al. 1997, Vasconcelos et al. 1997). After the identification of the Sin Nombre virus, which belongs to the family Bunyaviridae, as the etiologic agent of HPS, eight hantavirus subtypes and about 16 serogroups, each with a specific wild host, were identified (Bouloy & Zeller 2000). In the case of the American hantaviruses, these hosts belong to the order Rodentia, family Muridae, subfamilies Sigmodontinae, Arvicolinae (Microtus pennsylvanicus related to Prospect hill virus) and Murinae (Rattus norvegicus that transmits Seoul virus, Pereira 1999). Rodents become chronically infected and excrete the virus for several weeks through saliva, feces and urine. In addition, viral antigen has been detected in different organs of these animals, mainly lungs, spleen, liver and kidney (Green et al. 1998). Recent phylogenetic studies have shown amazing superposition of mitochondrial DNA among hantaviruses and their wild hosts, demonstrating the co-evolution of these two species throughout millions of years (Zhao & Hay 1997) and human hantavirus infection is probably very old, but remained unrecognized as a nosologic entity for a long time. Humans are infected through inhalation of aerosols contaminated with saliva, feces or urine of the rodent host. Other routes of infection such as rodent bites and contact between humans are less likely (Le Gueno 1998). Alterations in the equilibrium of rodent populations and in their interaction dynamics with humans determine the occurrence of hantavirus outbreaks, a situation favored by the large and severe changes in the ecosystem during the last decades (climate changes, deforestation accompanied by the introduction of agricultural practices in these areas, etc.) (Figueiredo et al. 2001). In Brazil, 171 cases had been notified by the end of 2001 (data obtained from the National Health Foundation) in different states: Paraná (59 cases), Minas Gerais (19), São Paulo (28), Rio Grande do Sul (23 cases), Santa Catarina (22), Mato Grosso (14), Pará (2), and Maranhão, Bahia, Rio Grande do Norte and Goiás (1 case each). In Ribeirão Preto, São Paulo, eight cases were reported during the last few years and in the Triângulo Mineiro Region, several cases were observed in Uberlândia and, more recently, in Uberaba (Figueiredo et al. 2001, Ferreira et al. 2001, Silva-Vergara et al. 2001). We describe here the clinical-epidemiological profile of patients with HPS. POPULATION AND METHODS
The present study was conducted on eight patients diagnosed with HPS in Uberaba between April 2000 and April 2001. The diagnosis was confirmed by the detection of IgM antibodies against Sin Nombre virus by ELISA (Ksiazek et al. 1995) or immunohistochemistry using the alkaline phosphatase envision method (Zaki et al. 1995), carried out at Instituto Adolfo Lutz, São Paulo. Four cases were seen at private hospitals in the city, two of them by one of the authors in the final phase, and the respective clinical-epidemiological and evolutive data were obtained from the medical records. The other four patients were followed up at the Clínica de Doenças Infecciosas e Parasitárias, Hospital Escola, Faculdade de Medicina do Triângulo Mineiro, Uberaba, Minas Gerais. RESULTS
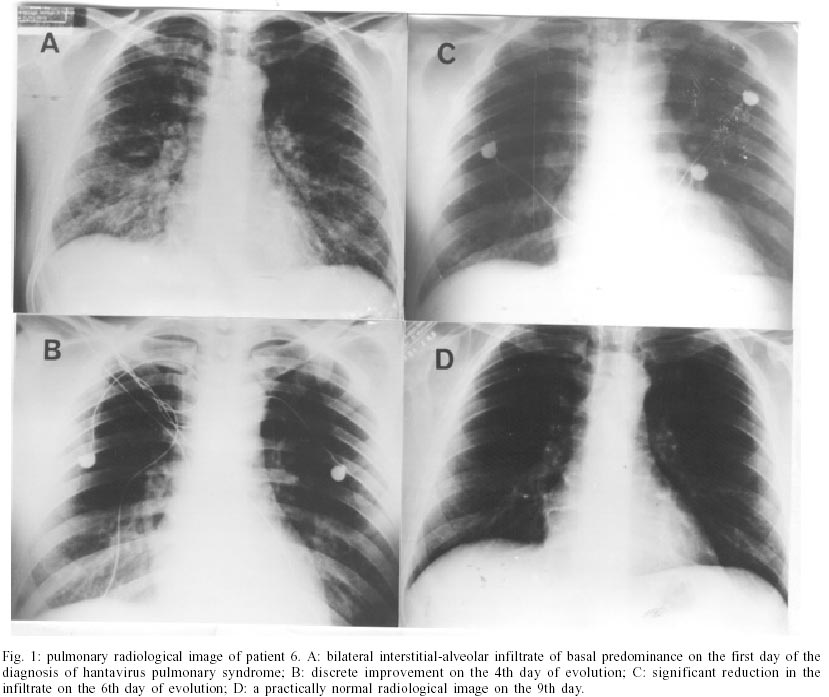
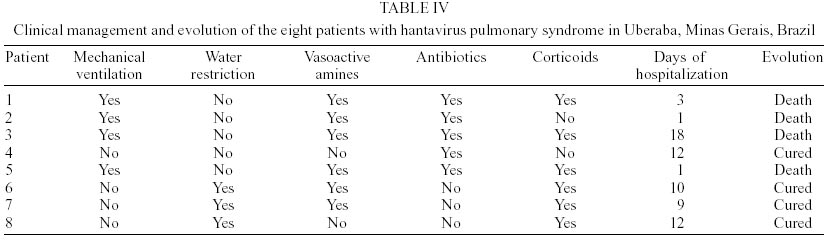
Some epidemiological data of the eight patients with HPS are reported in Table I. A positive history of contact with rodents was present in 100% of the cases. The search for rodents was carried out in five different localities of possible contact of the last four different cases, and species were captured (Bolomys lasiurus, Colomys tener e Oligoryzomys sp.). All of them were negative for hantavirus. However, 87 rats were captured around the house of patient 3, with 10 (8.7%) B. lasiurus rats (rat with a hairy tail) being positive for Sin Nombre hantavirus antibodies. Virus isolation was not performed in any case (Written information obtained from the Municipal Zoonosis Section). Evolution of symptoms was on average 3.6 days from the onset of symptoms to hospitalization. All patients showed very similar clinical signs and symptoms of the disease (Table II). Laboratory findings were suggestive of HPS in all of them (Table III). Radiological evaluation showed a bilateral interstitial-alveolar infiltrate in all cases (Figure). The clinical management and evolution of these patients can be observed in the Table IV. The hospitalization period ranged from one day (patients 2 and 5 who arrived in a state of shock and died) to 18 days in the case of patient 3, who presented several clinical problems such as arterial thrombosis, renal failure and sepsis secondary to nosocomial infection, which eventually led to her death. In this case post-mortem examination was not carried out. The diagnosis of hantavirus infection was confirmed by immunohistochemistry of a lung fragment in patient 1, serology and immunohistochemistry of the same organs in patient 2, and only by serology in the other six patients. DISCUSSION
The first confirmed case of HPS in Uberaba occurred in April 2000. Cases presenting closely similar ecoepide-miological characteristics have been previously observed in Uberlândia, MG, and in Ribeirão Preto, SP, which are located 100 and 176 km from Uberaba, respectively (Figueiredo et al. 1999, Ferreira et al. 2000). The history of the patients reported here permitted the identification of previous contact with rodents under different circumstances related to work (patients 1, 2, 4, 5 and 8), peridomicile (patient 3) or leisure (patients 6 and 7), with the last two patients reporting habitual fishing activity. This fact led to the establishment of an incubation period of 10 and 15 days, respectively, for the last two cases that passed the weekend in ranches (closed during the week) in different place and time on the riverbank where rodents were present. This observation is in accordance with the recently described incubation time of 9 to 33 days (Young et al. 2000). For the other patients, the precise incubation period could not be established. An investigation about the contacts of the last four cases has been initiated, but serology was not performed. No one presented any symptom of the infection, except an occupational contact of patient no. 8 that had febrile syndrome without any other signs, nor symptoms. This contact presented only positive ELISA IgG for Sin Nombre virus. The finding of B. lasiurus infected with hantavirus in the urban peridomicillary area of patient 3 suggests transmission in this local, and establishes epidemiological link between them. The present cases were recorded between March and September, with the disease occurring between March and July in six individuals, although most cases in Brazil, during the last two years, were diagnosed between July and December. This fact would define a different pattern of seasonality unlike as previously described for North America (Van Bevern 2000). The period from the onset of symptoms to the time of consultation was on average 3.6 days, similar to the time interval observed by others (Le Gueno 1998), and the clinical manifestations showed invariable uniformity (Table II). The respiratory picture, characterized by dry or discretely productive cough, rapidly progressing tachypnea and dyspnea, cyanosis, and a PO2 < 60 mmHg in all cases, together with the radiological findings of a bilateral interstitial-alveolar infiltrate corresponding to non-cardiogenic pulmonary edema secondary to pulmonary endothelial lesion, definitely characterized HPS in these patients (Le Gueno 1998). In addition, arterial hypotension was present in four of the eight patients, and in two patients shock was diagnosed at the time of consultation, demonstrating the cardiovascular repercussions observed for this syndrome (Figueiredo et al. 2001). The main laboratory alterations classically described in HPS (Van Bevern 2000) were present in all but one (Table III) and creatinine levels were found to be altered in six patients, confirming other studies on renal injury in HPS described in humans and rodents, with these changes being due to both hypotension and renal endothelial lesion (Green et al. 1998). Patients 1, 2, 3 and 5, seen at private centers, received mechanical ventilation, vasoactive amines and antibiotics due to the initial diagnosis of sepsis. These patients were not submitted to water restriction and three of them received corticoids. Hantavirus infection was suspected in these four patients during the final events preceding death. Patients 4, 6, 7 and 8 were seen at the Clínica de Doenças Infecciosas e Parasitárias, Hospital Escola, Faculdade de Medicina do Triângulo Mineiro, Uberaba, Minas Gerais. Patients 6 and 7 were admitted to the Intensive Care Unit and patients 4 and 8 were hospitalized at the Hospital Isolation Unit of the Infectious Diseases Clinic due to the lack of beds in the ICU. The epidemiological, clinical and laboratory characteristics of these patients were similar to those of the four patients discussed above. None of them received mechanical ventilation, two required vasoactive amines and only one of the four received antibiotics, although the presumptive diagnosis of hantavirus was made at the beginning. Three of the four patients who survived were treated with corticoids, although the real benefit of this therapy is controversial, and water restriction was prescribed to the last three. All four patients survived. The mortality rate was 50% for this small series of patients, in agreement with the general trend observed during the last few years in Brazil and other places, showing a higher survival, as physicians become familiarized with the clinical approach to this syndrome (Ferreira et al. 2001). Due to the small number of patients, it is difficult to establish any relationship between survival and the characteristics of treatment. However, there is no doubt that respiratory and cardiovascular support and adequate water control are fundamental for the clinical management of the disease.
ACKNOWLEDGMENT
To Maria Rita de Souza for preparation of the manuscript. REFERENCES
Copyright 2002 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc02150t1.jpg] [oc02150t3.jpg] [oc02150t4.jpg] [oc02150t2.jpg] [oc02150f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}